

| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Original Article
Volume 12, Number 4, August 2019, pages 198-202
Intra-Esophageal pH Monitoring on Two Consecutive Days in Patients With Gastroesophageal Reflux Symptoms
Andrea de Oliveira Batistaa, Adriana Zanoni Dottia, Lilian Rose Otoboni Aprilea, Roberto Oliveira Dantasa, b
aDepartment of Medicine, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto, SP, Brazil
bCorresponding Author: Roberto Oliveira Dantas, Department of Medicine, Ribeirao Preto Medical School, University of Sao Paulo, Av. Bandeirantes 3900, Ribeirao Preto, SP 14049-900, Brazil
Manuscript submitted May 21, 2019, accepted June 20, 2019
Short title: Esophageal pH Evaluation on Two Days
doi: https://doi.org/10.14740/gr1189
| Abstract | ▴Top |
Background: The best method to measure the frequency and duration of gastroesophageal reflux is 24-h pH or 24-h pH/impedance monitoring. However, the detection of reflux can vary when measured on different days. Our aim was to evaluate the possibility that the severity of gastroesophageal reflux is different even under similar conditions on two consecutive days.
Methods: We performed a 48-h pH monitoring in 12 subjects, aged 25 - 63 years, who complaint of heartburn and regurgitation, ten with esophagitis and two with non-erosive disease. The pH measurement was conducted at 5 cm from the lower esophageal sphincter. The patients stayed at the Clinical Investigation Ward of the hospital for 48 h. On each day, they consumed a 2,000 calorie diet. The results obtained on the first day were compared with those on the second day.
Results: Mean reflux index in the upright position was different between the two days. Results of the pH-monitoring within the 2 h after the meal revealed differences in the number of acidic reflux and reflux index episodes. Three patients had abnormal DeMeester score on one day and normal score on the other day. Considering the upper limit of 6.0% of the test duration with esophageal pH < 4 as indicative of gastroesophageal reflux disease, two patients showed abnormal results on one day and normal results on the other day.
Conclusions: The 24-h pH monitoring, performed on two consecutive days under similar conditions, can lead to different diagnosis of gastroesophageal reflux disease in symptomatic patients.
Keywords: Esophagitis; Gastroesophageal reflux disease; Esophagus; Heartburn; Regurgitation
| Introduction | ▴Top |
Gastroesophageal reflux symptoms are frequent in the population, which significantly influence quality of life [1]. There has been an increase in the prevalence of gastroesophageal reflux disease (GERD) [2]. Patients complaining of heartburn and acid regurgitation, the most frequent symptoms of GERD, who seek medical care at public or private healthcare centers should undergo a series of tests following the clinical examination for proper diagnosis [3].
The symptoms of heartburn and regurgitation are not sensitive enough to make the diagnosis of GERD [4]. However, if patients do not have alarm symptoms, such as anemia, weight loss, dysphagia and bleeding, they can be treated for GERD and evaluated for the treatment response. The first diagnostic test of GERD is upper gastrointestinal endoscopy [3-6], which has a high specificity (90-95%) for the disease, despite a low sensitivity (50%) [4]. Upper gastrointestinal endoscopy can detect mucosal alterations characteristic of the disease and its complications, including esophageal strictures or Barrett esophagus, and other diseases such as eosinophilic esophagitis and cancer. When no mucosal changes suggestive of erosive GERD are detected by endoscopy, the diagnosis of non-erosive reflux disease (NERD) should be considered. Following endoscopy, an esophageal pH monitoring or pH-impedance monitoring is recommended [3-6]. The test allows pH recordings during a longer period (24 h or 48 h) and indicates the presence of increased esophageal acid exposure.
Intra-esophageal pH monitoring is usually performed during a 24-h period. During this period, it is expected that reflux episodes occur in a similar frequency that of everyday life. However, this may vary depend on diet, stress, physical activity, and behavior, and hence symptom intensity tends to vary accordingly.
In this investigation, we tested the hypothesis that 24-h esophageal pH monitoring performed on two consecutive days yields different results, even under the same experimental conditions. To test this hypothesis, we measured intra-esophageal pH during 48 h under similar conditions in 12 patients with gastroesophageal reflux symptoms.
| Material and Methods | ▴Top |
Subjects
The 48-h intra-esophageal pH monitoring was performed in 12 patients (10 men) aged 25 to 63 years (mean 38.5 ± 12.0 years; median 36 years). Body mass index (BMI) varied from 17.6 kg/m2 to 39.3 kg/m2 (mean of 27.3 ± 2.0 kg/m2; median 27.1 kg/m2). All patients reported heartburn and regurgitation for more than 6 months and were in irregular use of proton bomb inhibitors. The symptoms were evaluated using the health-related quality of life questionnaire (HRQL) proposed by Velanovich et al [1] translated to Portuguese [7]. All patients underwent upper digestive endoscopy, which indicated that three patients had esophagitis Los Angeles (LA) classification [8] grade A, five LA-B, one LA-C, one LA-D and two patients had NERD [3]. They did not eat a special diet and did not have intense or regular physical activity.
The investigation was approved by the Human Research Committee of the University Hospital of Ribeirao Preto Medical School, IRB number 12220/2016.
pH monitoring
Intra-esophageal pH monitoring tests started in the morning after 6-h fast. All participants were instructed to stop treatment with H2 blockers or proton pump inhibitors at least 7 days prior to the study day. First, patients were submitted to esophageal manometry to establish the distance from the nostril to the superior border of the lower esophageal sphincter (LES). Manometric examination was performed using a water perfusion system (Alacer Biomedica, SP, Brazil) composed of an eight-lumen catheter, which was positioned to measure the intra-esophageal pressure at the LES and at 5, 10, 15 and 20 cm from the LES. Each patient performed 10 swallows of 5 mL bolus of water at room temperature in the supine position. The LES pressure was measured by the station pull-through technique. After assessment of esophageal contractions and LES pressure and confirmation of LES position, the manometric catheter was withdrew and a previously calibrated pH catheter (Alacer Biomedica, SP, Brazil) was introduced via the nostril. This catheter had a distal pH sensor which was placed 5 cm from the upper border of the LES. After the pH catheter localization patients were taken to the Clinical Investigation Ward of the hospital, where they stayed for 48 h. Patients were offered meals according to a pre-established schedule: 8:30 am-breakfast, 12:00 (noon)-lunch, 3:00 pm-snack, 6:30 pm-dinner, 9 pm-snack. The patients consumed about 2,000 calories in 24 h, containing 273 g of carbohydrate, 85 g of protein and 68 g of fat. Although the foods consumed were not the same in the two days, the total amount of carbohydrates, proteins, fats and energy was not significantly different between the two days. All meals were prepared by the division of nutrition of the hospital.
The pH recordings started after positioning of the sensor tip in esophageal distal segment. Esophageal pH was measured continuously for approximately 48 h. During the test, each participant reported the time and duration of the meals, the time they were in supine and in upright positions, as well as symptoms during the examination. They did not take any medication during the pH monitoring test.
Measurements
At the end, the results were downloaded to a computer and analyzed. The 48-h recordings were divided in two periods (first and second days), of approximately same duration, and the breakfast was used as the starting point of each day. Reflux was considered when the intra-esophageal pH dropped below 4. The number of reflux, and long reflux episodes (longer than 5 min), duration of the longest reflux, total duration of reflux, percentage of time with reflux, reflux index (number of reflux episodes per h), esophageal clearance, DeMeester index, and the number of refluxes within 2 h after the meals (post-meal reflux) [9, 10] were measured. A DeMeester index less than 14.7 and a percentage of time with a pH < 4 less than 6.0% of the test (Lyon Consensus [11]) were considered normal.
All patients consumed only the food provided by the Division of Nutrition of the hospital. They were allowed to walk around the ward or stay in the room as they choose.
Statistical analyses
Esophageal pH monitoring results were compared between the first day and the second day. Statistical analysis was performed by the statistical consulting company ProEstat Estatistics and Research (Ribeirao Preto, SP, Brazil). A linear model with mixed effects (random and fixed effects) [12], controlled by the duration of the test, was used for analysis. Time with reflux, reflux index and the DeMeester score were statistically evaluated by the Student’s t-test. In the tables, the results are shown as mean, standard deviation (SD) and median. A P ≤ 0.05 was considered to be significant.
| Results | ▴Top |
The manometric examination revealed hypotensive LES (pressure below 10 mm Hg) in 10 patients, and ineffective esophageal motility (non-peristaltic or hypotensive contractions) in three patients.
The HRQL score ranged from 15 to 47 (out of a maximum score of 50, with means severe symptoms as a group), with a mean of 32.3 (8.6), and median of 33.5.
The measurements showed that the mean reflux index in the upright position was different between the two days (Table 1). In addition, pH measurements performed within 2 h after a meal showed differences in the mean number of acidic reflux episodes and in the mean reflux index (Table 2).
 Click to view | Table 1. Gastroesophageal Acidic Reflux on Two Consecutive Days in Patients With Gastroesophageal Reflux Symptoms |
Click to view | Table 2. Gastroesophageal Acidic Reflux During 2 h After Meal on Two Consecutive Days |
The DeMeester score was 57.2 (49.60), median 39.5, on the first day, and 55.0 (40.8), median 39.5, on the second day (Fig. 1, P = 0.88). The percentage of time the intra-esophageal pH was < 4 was 15.5 (13.5)%, median 10.0%, on the first day, and 15.5 (12.0)%, median 11.5%, on the second day (Fig. 2, P = 0.99). Three patients had a DeMeester score higher than normal values (154.1, 33.8 and 19.9) on a day, but a normal score (13.1, 13.6, and 6.1) on the other day, the abnormal scores on the first day in one patient and on the second day in two patients. There was no relationship between normal or abnormal score and the time the patient was in the supine or upright position during the test or meal duration. Considering the percentage of time the patient had an esophageal pH < 4, in two patients this percentage was abnormal (> 6.0% of test duration) on a day and normal (< 6.0% of test duration) on the other day (42.9% and 9.7% on a day and 3.5% and 4.0% on the other), the abnormal score on the first day in one patient and on the second day in another.
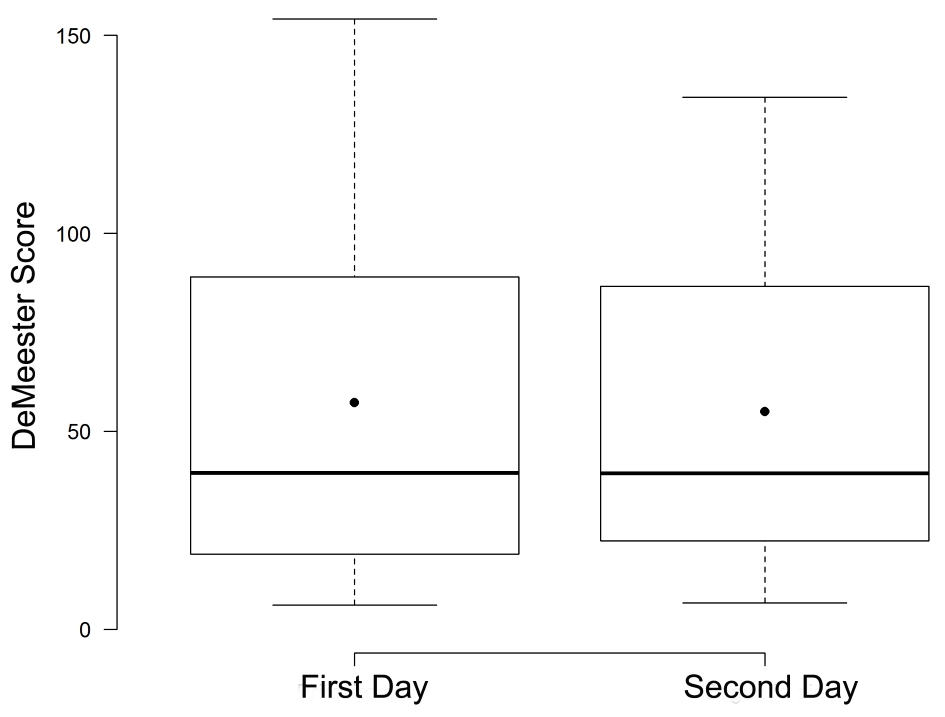 Click for large image | Figure 1. Box plot of the DeMeester score on the two consecutive days. No difference in mean and median scores was found between the days (P = 0.88). |
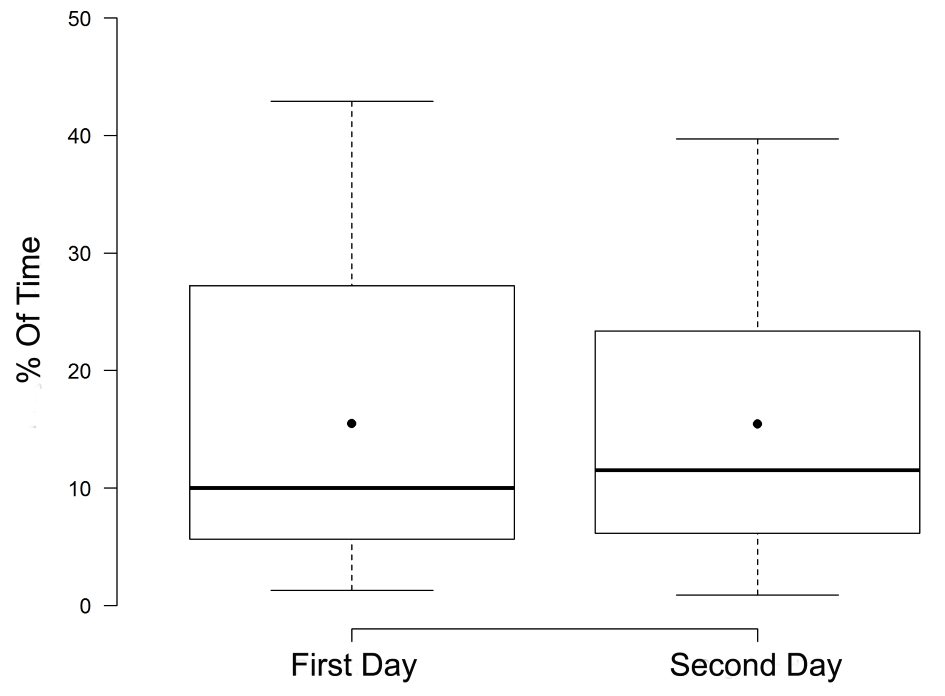 Click for large image | Figure 2. Box plot of the percentage of time with reflux on the two consecutive days. No difference in mean and median values was found between the two days (P = 0.99). |
| Discussion | ▴Top |
No clinical significant differences were found in mean pH monitoring results between the two days, although some individual differences were seen between the two days. The mean of the DeMeester score, which classifies patients into increased or normal risk for reflux, was similar on the two days. Also, the mean percentage of time the pH in esophagus was below 4 was almost the same. However, considering individual data, there was a great variation of results on the two days of monitoring. Normal and abnormal values for the DeMeester score were observed on the first or second day in three (25%) patients, and the same was observed for the percentage of time the pH was below 4 in two patients (17%).
Gastroesophageal reflux severity can be influenced by several factors including obesity, genetics, diet, ageing, body position, physical activity and esophageal motility [2, 4, 13-15]. Some of these factors can also have an important influence on pH measurements on different days, such as diet and body position [4, 14].
Following an animal protein meal both acidic reflux and acid exposure time are increased during the first postprandial hour as compared with a vegetable protein meal, which may explain more symptom complaints after consumption of animal protein foods [14].
We did not find any association between the time the patient was in supine position on the two days and results of the DeMeester score. It is known that elevation of the head of the bed and left lateral position are associated with a decrease in reflux and symptoms in patients with GERD [15]. However, the number of patients with abnormal DeMeester score on the one day and normal values on the other day was small, which did not allow any conclusive findings on the influence of body position on esophageal pH.
Considering the time the pH was below 4 during the test, two patients had abnormal and normal values on different days. This method is the most reliable measurement for the diagnosis of GERD [16] with normal upper limit varying from 4.0-6.0% in the literature though [11, 16].
Although we tried to establish two identical test conditions on the two study days we found different results of the pH monitoring between the days in some patients. This finding suggests that the 24-h esophageal pH monitoring test may yield different results on different days in patients with GERD, indicating that the interpretation of this test results should be made with caution in clinical practice. While normal pH monitoring results may be seen in patients with GERD, it is possible that abnormal results may be found in patients with symptoms but without a diagnosis of the disease. Also, the possibility that the stress during the examination had an influence on the results cannot be excluded. The cause for the high DeMeester score in one patient during one day (154.1) was the long duration of reflux episodes during this day (42.9% of the monitoring duration).
During the study period the most important limitation imposed to patients was the placement of the pH catheter inside the nose. To avoid this limitation, the catheter-free pH-metry has been developed [4, 11, 16], which can reduce the discomfort of the patients during prolonged pH monitoring. Nevertheless, this method is expensive, requires endoscopy and is not frequently used for pH monitoring. In addition, on the two study days, the participants did not take any medication that may affect gastric acid production and spent two days quite similar regarding activities and diet. However, it is not easy to obtain the same conditions at home in terms of activities, diet, work and social life on the study day compared with patient’s real life.
This investigation has some limitations. The number of patients was small, but was enough to show that variations in pH under experimental conditions may be important.
In conclusion, 24-h pH monitoring performed on two consecutive days under similar conditions can lead to different diagnosis of GERD in symptomatic patients.
Acknowledgments
None to declare.
Financial Support
No funding was received.
Conflict of Interest
The authors declared no conflict of interest.
Informed Consent
Written informed consent was obtained from each participant and the anonymity of each patient was preserved.
Author Contributions
All authors participated in the design of the study, in collection, analysis and interpretation of data, in the writing of the manuscript and in making the decision to submit it for publication.
| References | ▴Top |
- Velanovich V, Vallance SR, Gusz JR, Tapia FV, Harkabus MA. Quality of life scale for gastroesophageal reflux disease. J Am Coll Surg. 1996;183(3):217-224.
- Yamasaki T, Hemond C, Eisa M, Ganocy S, Fass R. The changing epidemiology of gastroesophageal reflux disease: are patients getting younger? J Neurogastroenterol Motil. 2018;24(4):559-569.
doi pubmed - Kandulski A, Moleda L, Muller-Schilling M. Diagnostic investigations of gastroesophageal reflux disease: who and when to refer and for what test? Visc Med. 2018;34(2):97-100.
doi pubmed - Richter JE. The many manifestations of gastroesophageal reflux disease: presentation, evaluation, and treatment. Gastroenterol Clin North Am. 2007;36(3):577-599, viii-ix.
doi pubmed - Vaezi MF, Sifrim D. Assessing old and new diagnostic tests for gastroesophageal reflux disease. Gastroenterology. 2018;154(2):289-301.
doi pubmed - Fisichella PM, Andolfi C, Orthopoulos G. Evaluation of gastroesophageal reflux disease. World J Surg. 2017;41(7):1672-1677.
doi pubmed - Fornari F, Gruber AC, Lopes Ade B, Cecchetti D, de Barros SG. [Symptom's questionnaire for gastroesophageal reflux disease]. Arq Gastroenterol. 2004;41(4):263-267.
doi pubmed - Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, Johnson F, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999;45(2):172-180.
doi pubmed - Halpern LM, Jolley SG, Tunell WP, Johnson DG, Sterling CE. The mean duration of gastroesophageal reflux during sleep as an indicator of respiratory symptoms from gastroesophageal reflux in children. J Pediatr Surg. 1991;26(6):686-690.
doi - Meyer R, Fischer GB. [Association between gastroesophageal reflux and dips in the oxygen transcutaneous saturation of the hemoglobin in infants with chronic obstructive ventilatory disease]. J Pediatr (Rio J). 2001;77(2):89-95.
doi - Gyawali CP, Kahrilas PJ, Savarino E, Zerbib F, Mion F, Smout A, Vaezi M, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018;67(7):1351-1362.
doi pubmed - Schall R. Estimation in generalized linear models with random effects. Biometrika. 1991;78:719-727.
doi - Martinucci I, de Bortoli N, Giacchino M, Bodini G, Marabotto E, Marchi S, Savarino V, et al. Esophageal motility abnormalities in gastroesophageal reflux disease. World J Gastrointest Pharmacol Ther. 2014;5(2):86-96.
doi pubmed - Martinucci I, Guidi G, Savarino EV, Frazzoni M, Tolone S, Frazzoni L, Fuccio L, et al. Vegetal and animal food proteins have a different impact in the first postprandial hour of impedance-pH analysis in patients with heartburn. Gastroenterol Res Pract. 2018;2018:7572430.
doi pubmed - Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med. 2006;166(9):965-971.
doi pubmed - Nasi A, Queiroz NSF, Michelsohn NH. Prolonged gastroesophageal reflux monitoring by impedance-phmetry: a review of the subject pondered with our experience with 1,200 cases. Arq Gastroenterol. 2018;55(Suppl 1):76-84.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.