aDepartment of Internal Medicine, Kawasaki Hospital, Kobe, Japan bDepartment of International Medicine, Kobe Tokushukai Hospital, Kobe, Japan cCorresponding Author: Nobuhiro Takeuchi, Department of Internal Medicine, Kobe Tokushukai Hospital, 1-3-10 Kamitakamaru, Tarumi-Ku, Kobe-shi, Hyogo 655-0017, Japan
Manuscript submitted April 3, 2017, accepted April 19, 2017 Short title: Pneumatosis Cystoides Intestinalis doi: https://doi.org/10.14740/gr834w
Intraperitoneal free air (IFA) is sometimes accompanied by pneumatosis cystoides intestinalis (PCI); therefore, proper diagnosis is essential for PCI management. We report two cases of PCI with IFA. A 70-year-old female taking anti-psychotic medication for schizophrenia presented with repeated vomiting and high-grade fever. Computed tomography revealed small, linear gaseous cysts in the intestinal wall along with IFA. Although there was no sign of peritoneal irritation, intestinal perforation was not excluded. Thus, exploratory laparotomy was performed; it revealed no ascites or perforated sites in the intestine, and revealed numerous small air bubbles in the intestinal wall and mesentery. Thus, a diagnosis of PCI was made, and ileostomy was performed to relieve intestinal pressure. The postoperative course was uneventful. A 79-year-old male with pulmonary emphysema presented with dyspnea due to abdominal distention. Cyanosis was evident, and arterial blood gas analysis revealed metabolic acidosis. CT revealed massive IFA along with multiple, small bubbly cysts under the intestinal serosa. He was intubated because of worsening respiratory conditions, and a 12-French drain was inserted to relieve the intraperitoneal pressure. There was no evidence of peritonitis, and IFA was conservatively observed.
Keywords: Pneumatosis cystoides intestinalis; Intraperitoneal free air
Pneumatosis cystoides intestinalis (PCI) is a rare condition in which multiple cysts are formed beneath the intestinal mucosa and serosa. The occurrence of PCI is related to lung diseases or anti-psychotic medication use because they increase airway or intra-intestinal pressure, thereby diverting air into the intestinal submucosa or seromucosa. PCI sometimes presents radiological findings identical to those of acute abdomen, including gastrointestinal perforation or intestinal necrosis. Here we present two cases of PCI presented with intraperitoneal free air (IFA).
A 70-year-old female with complaints of nausea, repeated vomiting, and high-grade fever was transferred to our hospital. She had been admitted to a psychiatric hospital for the treatment for schizophrenia and was taking risperidone 6 mg/day. Her medical history included cholecystitis, which had been laparoscopically treated 20 years ago. Upon arrival, her blood pressure was 88/65 mm Hg, heart rate was 48 beats/min, body temperature was 39.8 °C, respiratory rate was 18/min, and percutaneous oxygen saturation was 92% under 4 L/min oxygen inhalation. Inspection of the palpebral conjunctiva revealed no evidence of anemia. Auscultation of the heart revealed no murmurs, and auscultation of the lungs revealed no rales or other lung sounds. Her abdomen was remarkably distended without tenderness and peritoneal irritation.
Blood biochemistry revealed increased white blood cell (WBC) (15,940/μL) and red blood cell (486 × 104/μL), elevated hemoglobin level (15.6 g/dL), elevated hematocrit (47.8%), impaired liver enzymes (aspartate aminotransferase (137 IU/L (13 - 37 IU/L)) and alanine aminotransferase (88 IU/L (8 - 45 IU/L))), elevated blood urea nitrogen level (44.9 mg/dL (7.8 - 18.9 IU/L)), increased serum sodium level (152 mEq/mL (138 - 146 mEq/mL)), and coagulation dysfunction (51% prothrombin time and 1.50 international normalized ratio of prothrombin time).
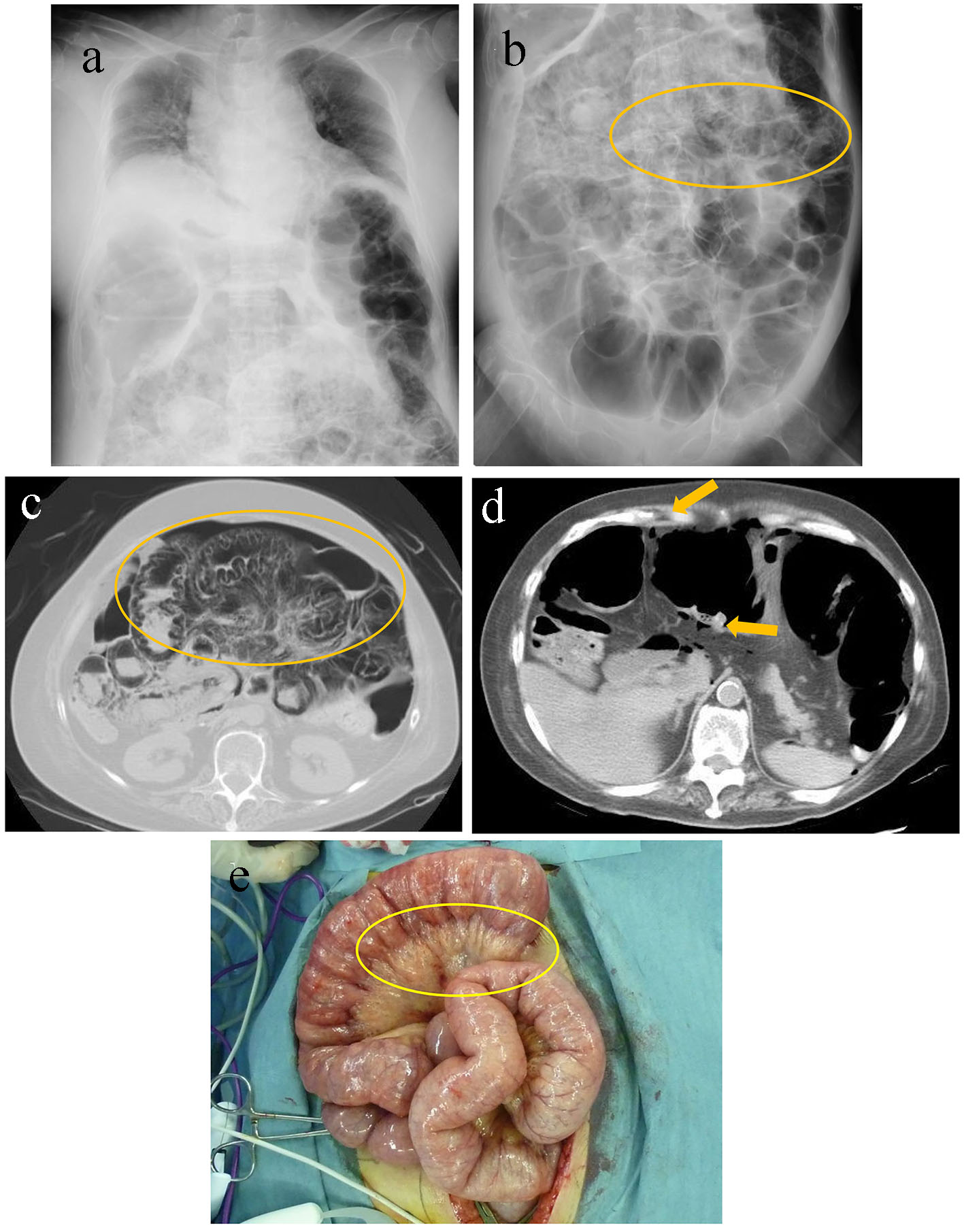
A chest radiography revealed elevation of the diaphragm due to dilated intestines (Fig. 1a). A radiography of the abdomen revealed diffusely dilated intestines and multiple small radiolucent linear bubbles that lined the intestines (Fig. 1b). An abdominal computed tomography (CT) revealed small, linear gaseous cysts in the intestinal wall (Fig. 1c) along with IFA (Fig. 1d).
Figure 1. A chest radiography revealed elevation of the diaphragm due to dilated and gaseous intestines (a). A radiograph of the abdomen revealed diffusely dilated intestines and multiple, small radiolucent linear bubbles lining the intestines (circle) (b). Abdominal computed tomography revealed dilated and gaseous small intestines, retention of gas in the intestinal wall (circle) (c), and intraperitoneal free air (arrows) (d). Operative findings revealed small air bubbles in the intestinal wall and mesentery (e).
From these findings, the possibility of gastrointestinal perforation could not be excluded because of fever and leukocytosis; thus, she was deemed a candidate for surgical examination. Her abdomen was opened using an abdominal midline incision under general anesthesia. A remarkably dilated ileum was observed at 120 - 200 cm from the Treitz ligament. Neither ascites nor apparent perforation sites were discovered. Numerous small air bubbles were found in the intestinal wall and mesentery (Fig. 1e). The patient was diagnosed with PCI, and ileostomy was performed to relieve the intestinal dilatation. Postoperative course was uneventful.
Case 2
A 79-year-old male presented with shortness of breath caused by abdominal distention and lower abdominal pain. He regularly visited a primary care physician for pulmonary emphysema, which was treated using home oxygen therapy. He had smoked two packs of cigarettes a day for 50 years until he was diagnosed with pulmonary emphysema. He reported drinking a bottle of whisky a day. Upon arrival, his blood pressure was 104/60 mm Hg, heart rate was 69 beats/min, body temperature was 37.1 °C, and respiratory rate was 42 breaths/min. His percutaneous oxygen saturation was 80% under 2 L/min oxygen inhalation. Physical examination revealed a remarkably distended abdomen without board-like rigidity or sign of peritoneal irritation. Auscultation revealed bilateral rhonchi in lungs. Cyanosis was evident on the entire body. With the worsening respiratory condition, he was intubated and admitted to the intensive care unit.
Blood biochemistry revealed mild inflammation, with a WBC count of 12,840/μL (90.0% neutrophils), and C-reactive protein level of 1.55 mg/dL (< 0.30 mg/dL); furthermore, mild hypoproteinemia (5.7 g/dL (6.7 - 8.3 g/dL)) and mild hypoalbuminemia (3.1 g/dL (4.1 - 5.2 g/dL)) were observed. An arterial blood gas analysis under 2 L/min oxygen inhalation revealed mild acidosis (pH 7.203, pCO2 46.8 mm Hg, pO2 65.3 mm Hg, HCO3- 17.7 mmol/L, and base excess -9.8 mmol/L).
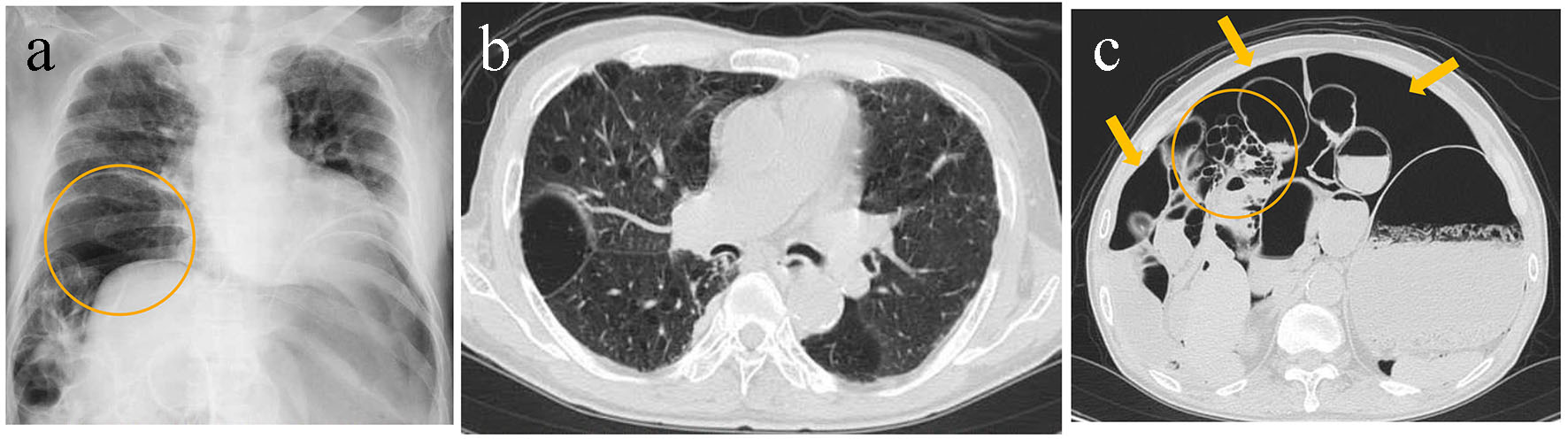
A chest radiograph revealed decompression of the right lung with elevation of the diaphragm and retention of massive IFA under the diaphragm (Fig. 2a). Non-contrast CT revealed bilateral dispersed emphysematous bullae in the lungs (Fig. 2b), distention of the small intestine, and IFA along with multiple, small bubbly cysts beneath the intestinal serosa (Fig. 2c) without the detection of ascites. Gastrointestinal perforation was considered as one of the differential diagnoses; however, it was rejected because of the absence of abdominal tenderness and peritoneal irritation. A 12-French drainage tube was inserted into his peritoneal cavity to deaerate the free air. Immediately after that, his symptoms, including abdominal distention, dyspnea and cyanosis of the entire body, rapidly alleviated. On day 2 of admission, his oxygenation improved and he was extubated. Gastrography was performed to check for perforation in intestines, revealing no apparent sites of perforation. After initiation of oral intake, none of the symptoms recurred. He was discharged on day 10 of admission.
Figure 2. A chest radiography revealed decompression of the right lung with an elevated diaphragm and the retention of massive free air under the diaphragm (circle) (a). Non-contrast computed tomography revealed bilateral multiple emphysematous bullae in the lungs (b), distended small intestines, and intraperitoneal free air (arrows) along with multiple, small bubbly cysts beneath the intestinal serosa (circle) (c).
PCI is a rare condition in which multiple gaseous cysts are formed beneath the intestinal mucosa and serosa due to a variety of diseases. PCI was first described in 1730 by Du Vernoi [1]. The number of males affected with PCI is 3.5-fold higher that of females. In approximately 85% of patients, PCI is associated with collagen diseases or chronic pulmonary diseases; approximately 15% of patients have no underlying disease. The occurrence of PCI is most common in the colon (47%), followed by small bowel (27%), stomach (5%), and both colon and small bowel (7%) [2].
The clinical manifestations of PCI are characterized by gastrointestinal symptoms, including vomiting or abdominal distension in patients with PCI in the small bowels, and by melena and diarrhea in patients with PCI in the large bowels [3]. In both of our presented cases, small bowels were affected; case 1 presented with vomiting, and case 2 presented with abdominal pain and distention. Physical examination of patients with PCI frequently reveals no signs of peritoneal irritation or muscle rigidity.
PCI is classified as primary or secondary based on its etiology. Primary PCI arises from unknown causes, whereas secondary PCI arises from gastrointestinal diseases, including gastroduodenal ulcers, pyloric stenosis, small bowel obstruction, appendicitis, ischemic or inflammatory intestinal diseases; lung diseases, including asthma or chronic obstructive pulmonary disease (COPD); and autoimmune diseases.
The pathophysiology of PCI can be explained by the following theories [4, 5]: 1) mechanical theory, 2) bacterial theory, 3) pulmonary theory, and 4) chemical theory. The mechanical theory suggests that there is an inflow of air through damaged mucosa, which is caused by intestinal obstruction, severe constipation, gastrointestinal ulcers, or intestinal necrosis, resulting in increased intestinal pressure. The bacterial theory suggests that there is an invasion of gas-producing bacteria, including the clostridium species, into intestinal submucosa, which produces gas in the intestinal walls. The pulmonary theory suggests that there is an inflow of gas into the peritoneal cavity, mesentery, and intestinal walls via the mediastinum from damaged alveoli due to increased intrathoracic pressure resulting from COPD or coughing. The chemical theory suggests that the cause is occupational and continuous exposure to trichloroethylene. PCI in case 1 presumably stemmed from continuous dilatation and increased pressure due to constipation or reduced peristalsis due to intake of an anti-psychotic drug; in case 2 it stemmed from alveolar air leakage secondary to high airway pressure due to COPD. The use of drugs, including α-glucosidase inhibitors, risperidone, and several other chemotherapeutic agents, is known to cause PCI by causing intestinal dilatation and paralysis [6-8].
PCI is diagnosed using imaging modalities (radiographs or CT). A radiograph of the abdomen shows multiple, small gaseous cysts that line the intestinal walls. CT shows multiple gaseous cysts within the intestinal walls. PCI is sometimes accompanied by IFA or portal venous gas [9, 10]. IFA occurs in approximately 15% of PCI cases in the small bowels and 2% of those in the large bowels [3]. In our presented cases, case 1 showed massive IFA and case 2 showed small amounts of IFA with multiple, small gaseous cysts within the small intestinal walls on CT. Notably in both cases, no ascites were observed on CT. The appearance of gaseous cysts on CT can be described as linear, circular, and bubbly; however, it is not helpful in determining the severity of PCI [11]. Case 1 presented with linear cysts and case 2 presented with bubbly cysts.
A principle treatment of PCI is conservative therapy regardless of the presence of IFA or portal venous gas unless there is an evidence of intestinal stenosis or bleeding. Surgical treatment is adopted if the clinical manifestation of intestinal necrosis is evident. Conservative treatment of IFA can be chosen if the following conditions are met: 1) low-grade fever, 2) spontaneous resolution of the abdominal pain, 3) possibility of decompression of the intestinal pressure, and 4) apparent (even if it is localized) presence of PCI. These conditions may suggest the absence of intestinal necrosis. Here, case 1 required emergency surgery to investigate the cause of IFA, revealing a remarkably dilated ileum without any apparent perforation sites in the intestines and intestinal necrosis. In case 1, PCI was considered to stem from chronic bowel dilatations caused by the use of anti-psychotic medication; exploratory laparotomy and ileostomy were effective in decreasing intra-abdominal pressure. Case 2 required emergency tracheal intubation because of a worsening respiratory condition caused by increased intra-abdominal pressure, followed by decompression of intraperitoneal gas using a drainage tube to aid in his oxygenation. As conservative therapies for PCI, high-flow oxygen therapy and oxygen inhalation therapy can be effective [12, 13]. Oxygen administration may help replace nitrogen with oxygen in intestinal pneumatosis; thus, pneumatosis disappears via concentration gradient. Oxygen may also help suppress the growth of anerobic intestinal bacteria that cause intestinal pneumatosis.
Conclusion
We reported two cases of PCI with IFA. The detection of IFA using imaging modalities may suggest intestinal perforation. However, IFA caused by PCI can be observed without surgical intervention or investigation. Clinicians should be aware that PCI is one of the differential diagnoses when IFA without ascites or signs of peritoneal irritation is present and that PCI can be observed using conservative treatment modalities.
Du Vernoi GJ. Aer intestinorun tam subextimaquam intima inclusus. Obsergationae Anatomicae Acad Scient Imp Petoropol. 1730;5:213-215
Morris MS, Gee AC, Cho SD, Limbaugh K, Underwood S, Ham B, Schreiber MA. Management and outcome of pneumatosis intestinalis. Am J Surg. 2008;195(5):679-682; discussion 682-673.
Jamart J. Pneumatosis cystoides intestinalis. A statistical study of 919 cases. Acta Hepatogastroenterol (Stuttg). 1979;26(5):419-422.
Galandiuk S, Fazio VW. Pneumatosis cystoides intestinalis. A review of the literature. Dis Colon Rectum. 1986;29(5):358-363. doipubmed
Heng Y, Schuffler MD, Haggitt RC, Rohrmann CA. Pneumatosis intestinalis: a review. Am J Gastroenterol. 1995;90(10):1747-1758. pubmed
Kasumoto H, Nariyama S, Yamamoto T, et al. A hemodialysis patient taking an oral α-glucosidase inhibitor who developed pneumatosis cystoides intestinalis accompanied by intra-abdominal free air. J Jpn Soc for Dial Ther. 2010;43(11):939-943. doi
Yamaguchi E, Uchida M, Yamamoto Y. Six cases of pneumatosis cystoides intestinalis (PCI) that improved with conservative treatment. J Jpn Soc Coloproctol. 2013;66(7):522-528. doi
Mimatsu K, Oida T, Kawasaki A, Kano H, Kuboi Y, Aramaki O, Amano S. Pneumatosis cystoides intestinalis after fluorouracil chemotherapy for rectal cancer. World J Gastroenterol. 2008;14(20):3273-3275. doipubmed
Kaya B, Celik K, Karip AB, Altun H, Ozbay Ozel N, Bat O, Memisoglu K. Pneumatosis cystoides intestinalis mimicking acute abdomen. Turk J Gastroenterol. 2014;25(4):426-428. doipubmed
Sakurai Y, Hikichi M, Isogaki J, Furuta S, Sunagawa R, Inaba K, Komori Y, et al. Pneumatosis cystoides intestinalis associated with massive free air mimicking perforated diffuse peritonitis. World J Gastroenterol. 2008;14(43):6753-6756. doipubmed
Ho LM, Paulson EK, Thompson WM. Pneumatosis intestinalis in the adult: benign to life-threatening causes. AJR Am J Roentgenol. 2007;188(6):1604-1613. doipubmed
Holt S, Gilmour HM, Buist TA, Marwick K, Heading RC. High flow oxygen therapy for pneumatosis coli. Gut. 1979;20(6):493-498. doipubmed
Down RH, Castleden WM. Oxygen therapy for pneumatosis coli. Br Med J. 1975;1(5956):493-494. doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.