Figures
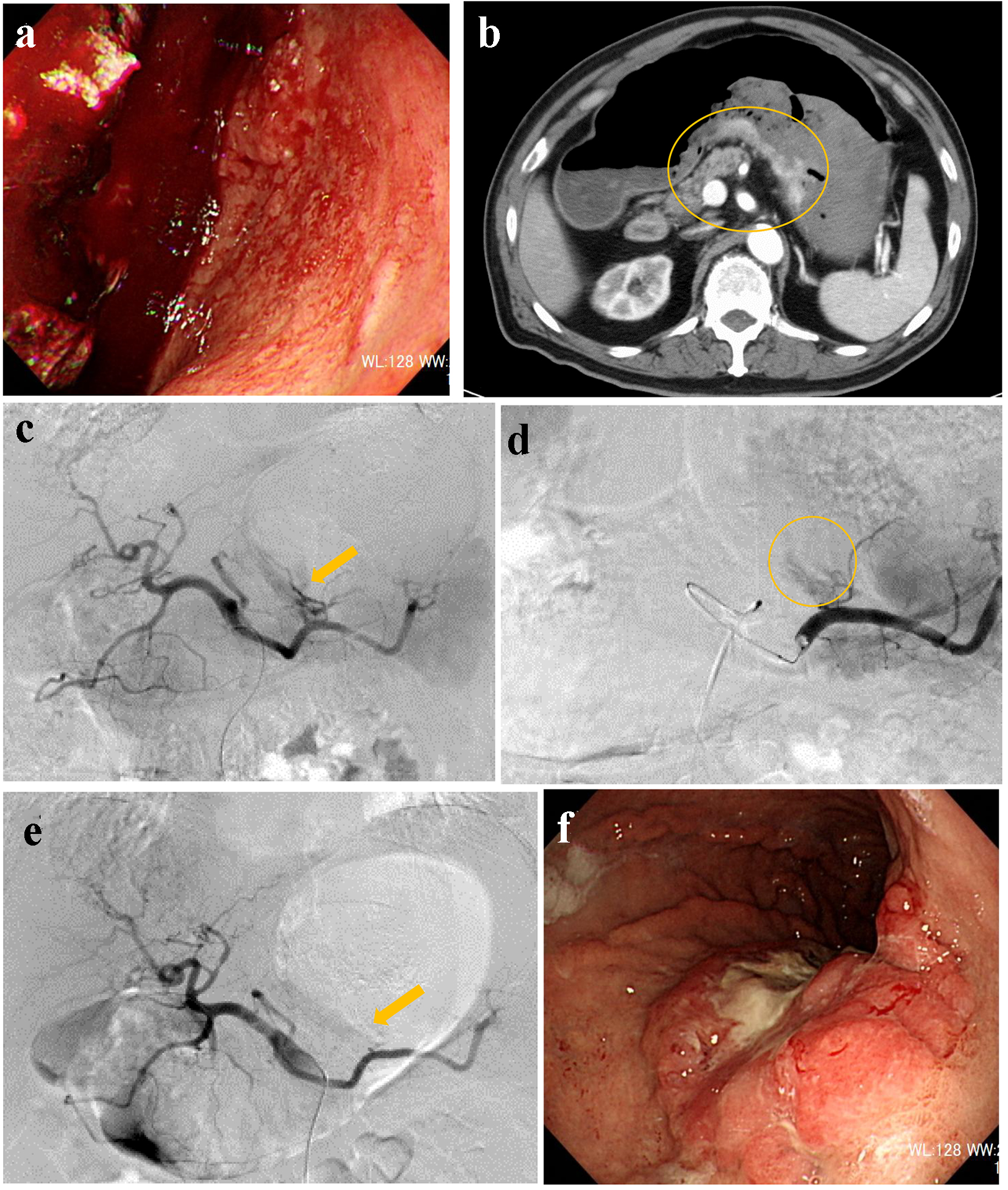
Figure 1. (a) Endoscopy reveals massive coagulated clots over the stomach. (b) Contrast-enhanced computed tomography suggests extravasation from the posterior walls of the lower stomach body (circle). (c) Angiography reveals extravasation from the posterior gastric artery (arrow). (d) A microcatheter is engaged into the branch of the posterior gastric artery (circle). (e) The responsible artery is successfully occluded by a gelatin sponge (arrow). (f) Endoscopy reveals Bormann 3 type cancer at the posterior walls of the lower gastric body.
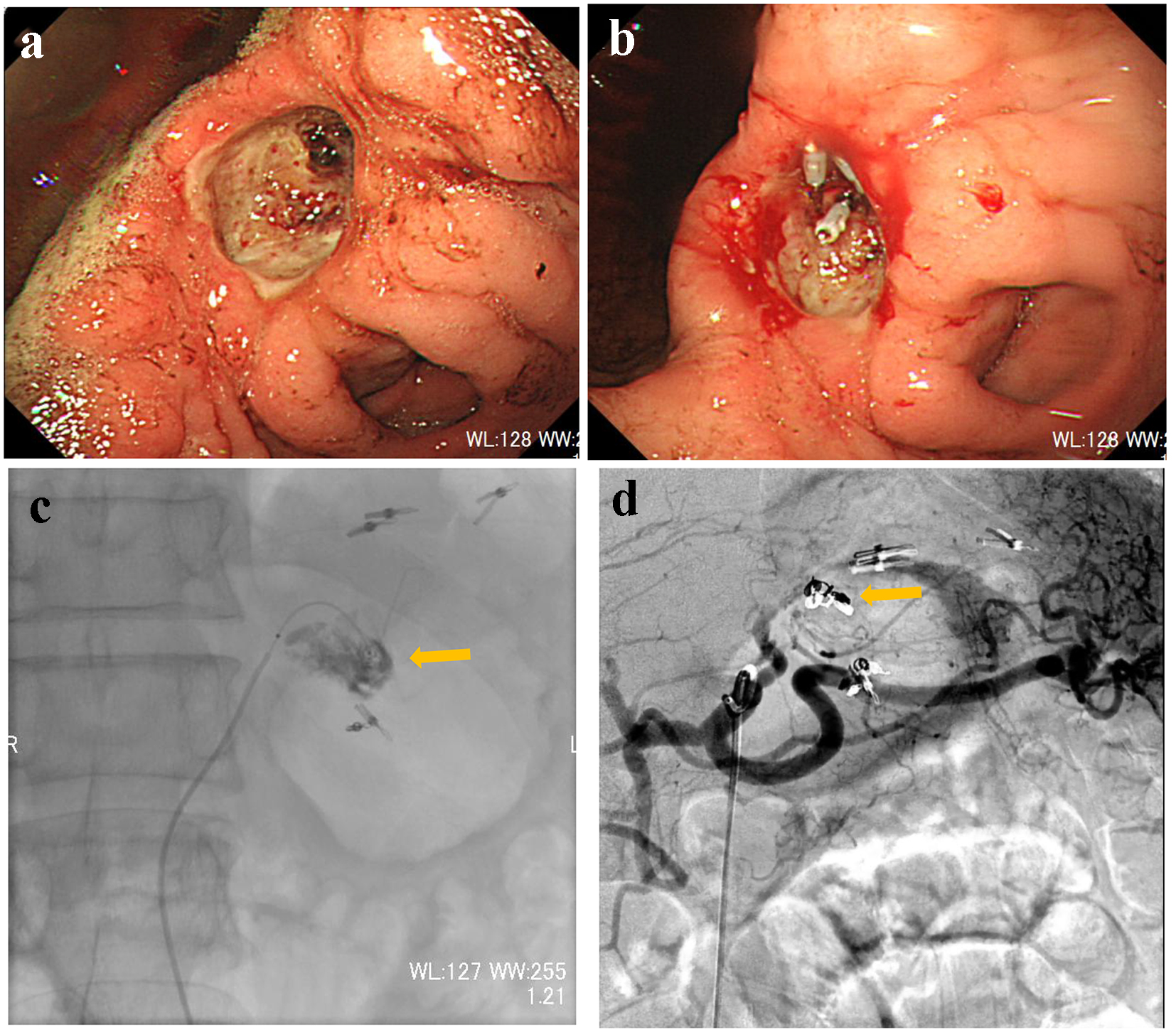
Figure 2. (a) Endoscopy reveals Bormann 2 type cancer with exposed vessels at the angle of the stomach. (b) The exposed vessels are staunched by endoscopic clips. (c) Contrast injection from a microcatheter advanced into the left gastric artery reveals extravasation (arrow). (d) The main trunk of the left gastric artery is occluded by microcoils (arrow).
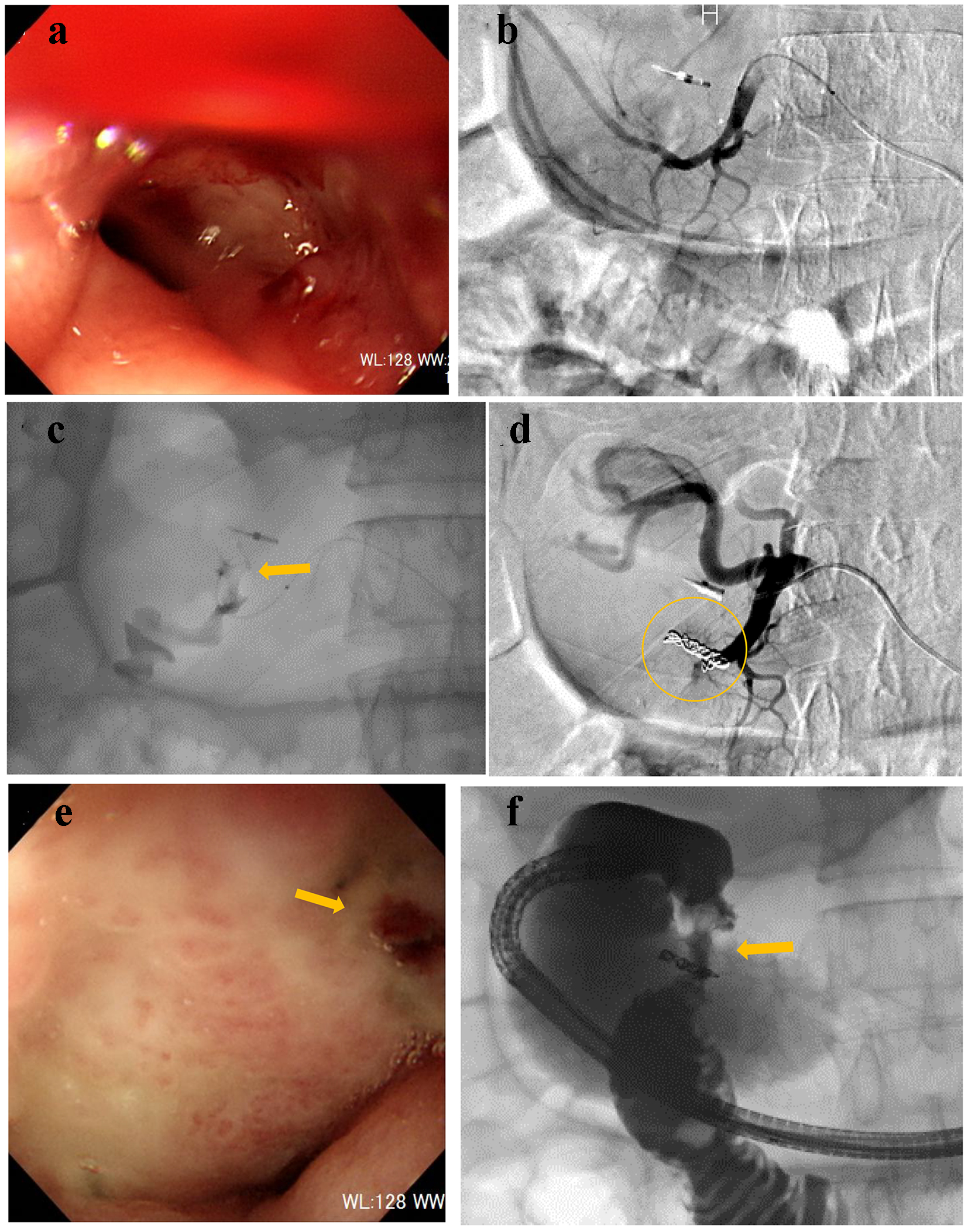
Figure 3. (a) Endoscopy reveals oozing at the duodenal bulb. (b) Gastroduodenal angiography reveals no extravasation. (c) Contrast injection from a microcatheter advanced into the right gastro-omental artery reveals extravasation (arrow). (d) The main trunk of the right gastro-omental artery is occluded by microcoils (circle). (e) Endoscopy confirms successful hemostasis (arrow). (f) Gastrography under endoscopy reveals the narrowed duodenal bulb (arrow).
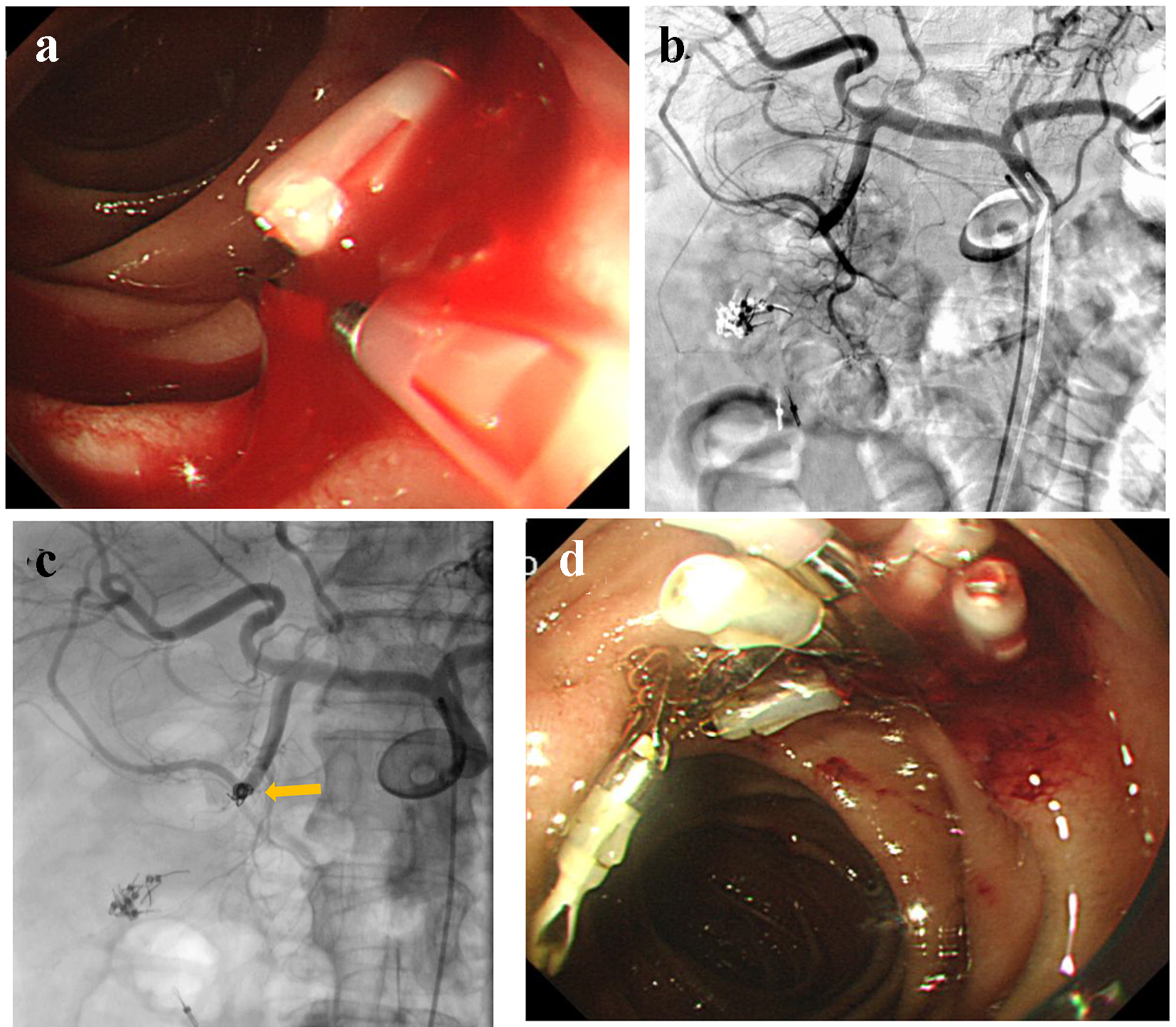
Figure 4. (a) An exposed vessel at the posterior walls of the descending duodenum is revealed and endoscopic hemostasis is attempted. (b) Gastroduodenal angiography reveals no evidence of extravasation. (c) Anterior superior pancreatico-duodenal artery is occluded by microcoils (arrow). (d) Endoscopy reveals successful hemostasis.
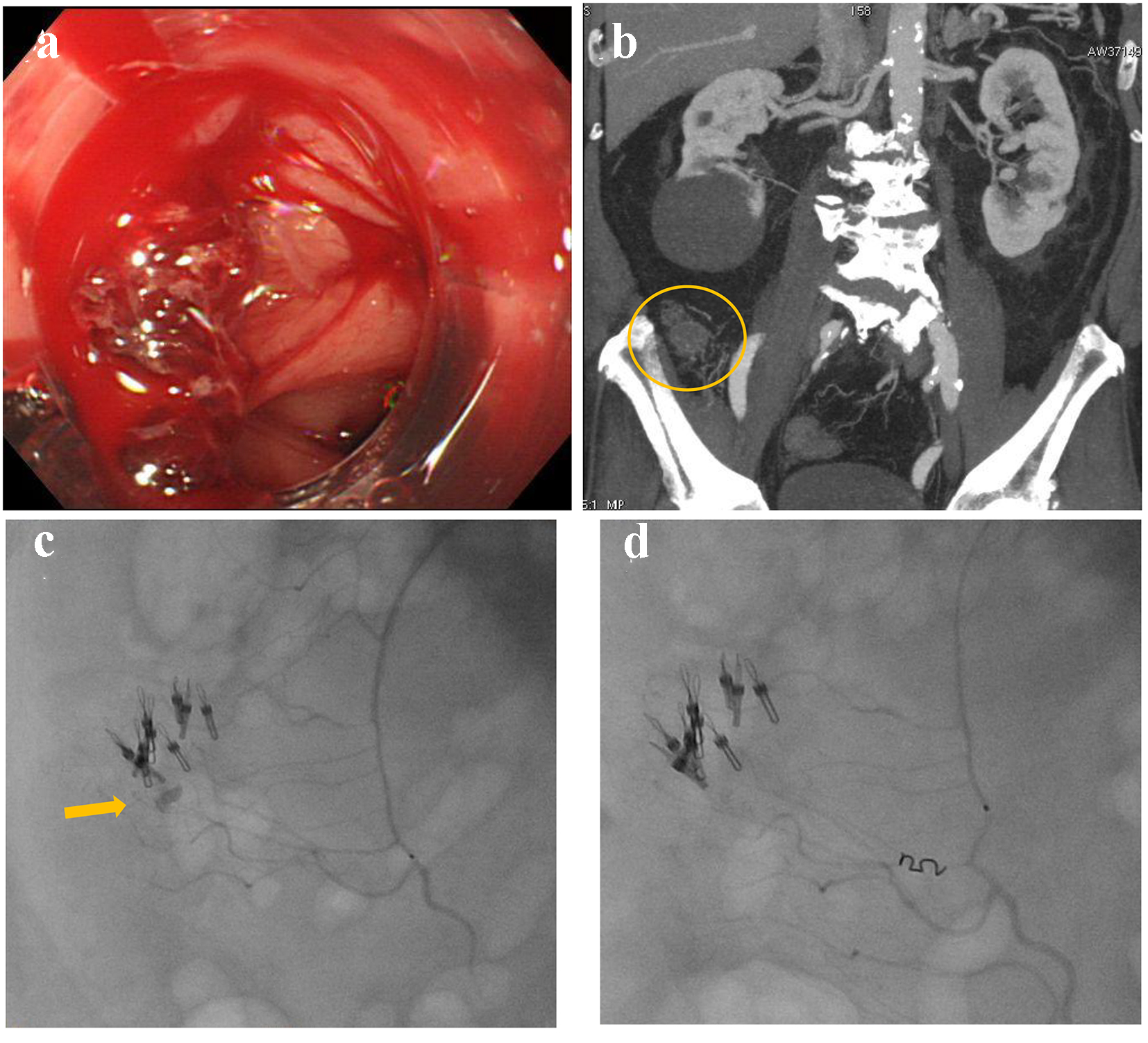
Figure 5. (a) Colonoscopy reveals multiple diverticulosis in the ascending colon with active bleeding. (b) Contrast-enhanced computed tomography reveals extravasation at the distal superior mesenteric artery (circle). (c) Contrast injection from a microcatheter reveals extravasation (arrow). (d) The distal superior mesenteric artery is occluded by a microcoil.
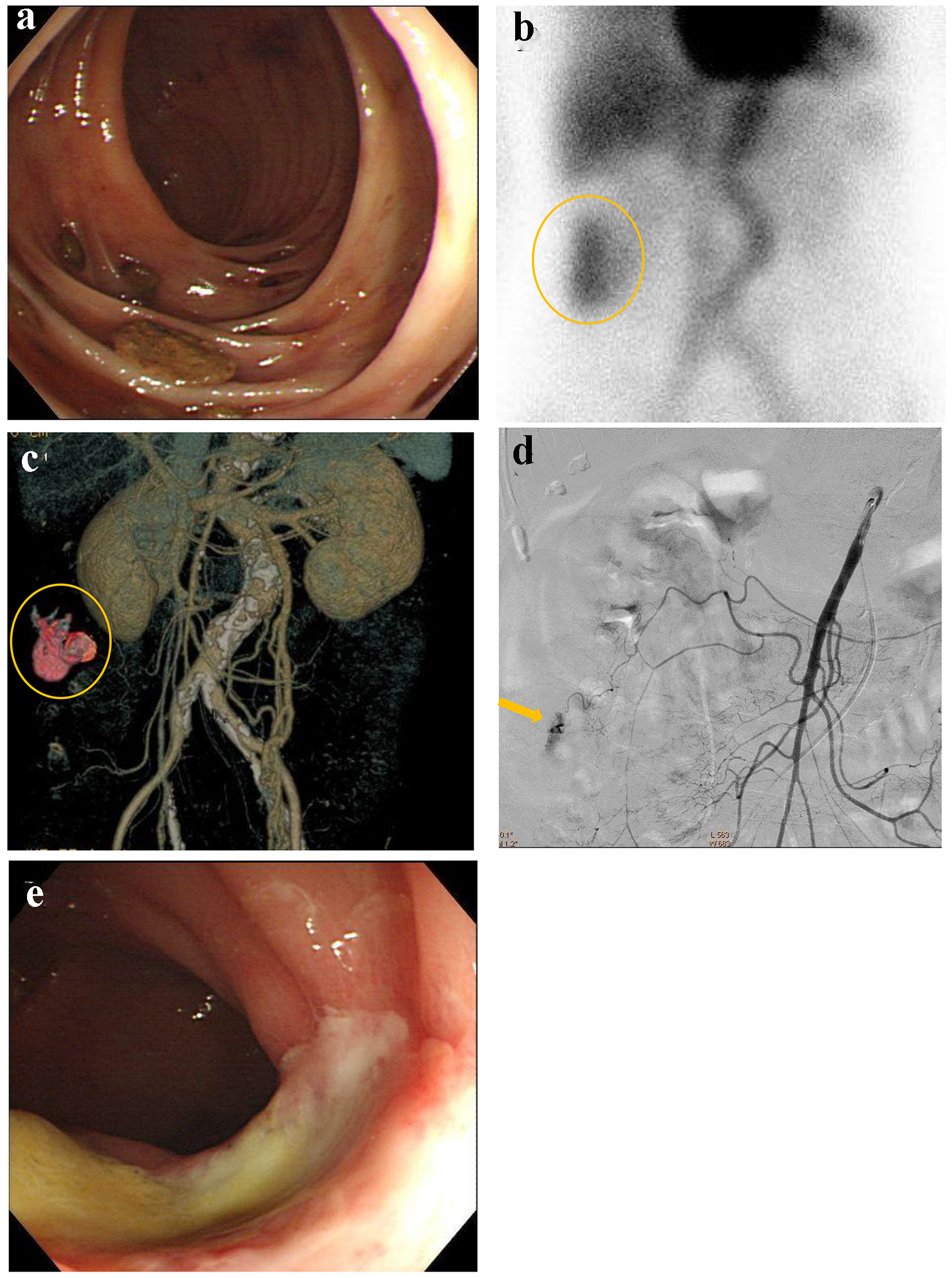
Figure 6. (a) Colonoscopy reveals multiple diverticulosis in the ascending colon without evidence of bleeding. (b) 99m-labelled red blood cell scintigraphy suggests the bleeding sites in the ascending colon (circle). (c) Contrast-enhanced computed tomography suggests extravasation at the middle of ascending colon (circle). (d) Superior mesenteric artery angiography reveals extravasation from the middle colic artery (arrow). (e) Colonoscopy reveals successful hemostasis and mild colonic ischemia.
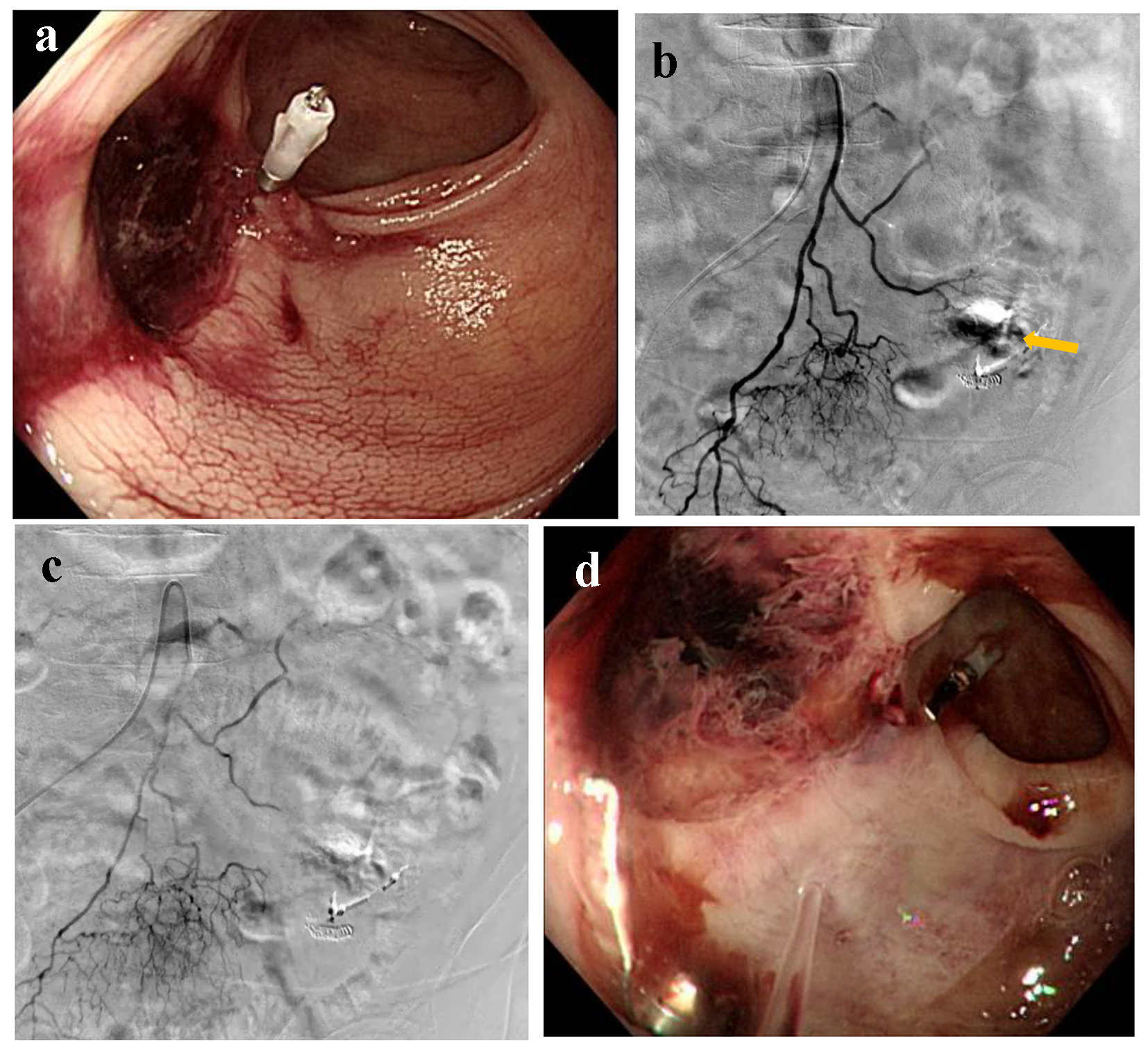
Figure 7. (a) Colonoscopy reveals ulcerative scars with a suspected exposed vessel at sigmoid colon 40 cm from anal canal without evidence of active bleeding. (b) Inferior mesenteric artery angiography reveals extravasation (arrow). (c) The distal inferior mesenteric artery is occluded by a gelatin sponge. (d) Colonoscopy reveals successful homeostasis with mild ischemic changes at sigmoid colon.