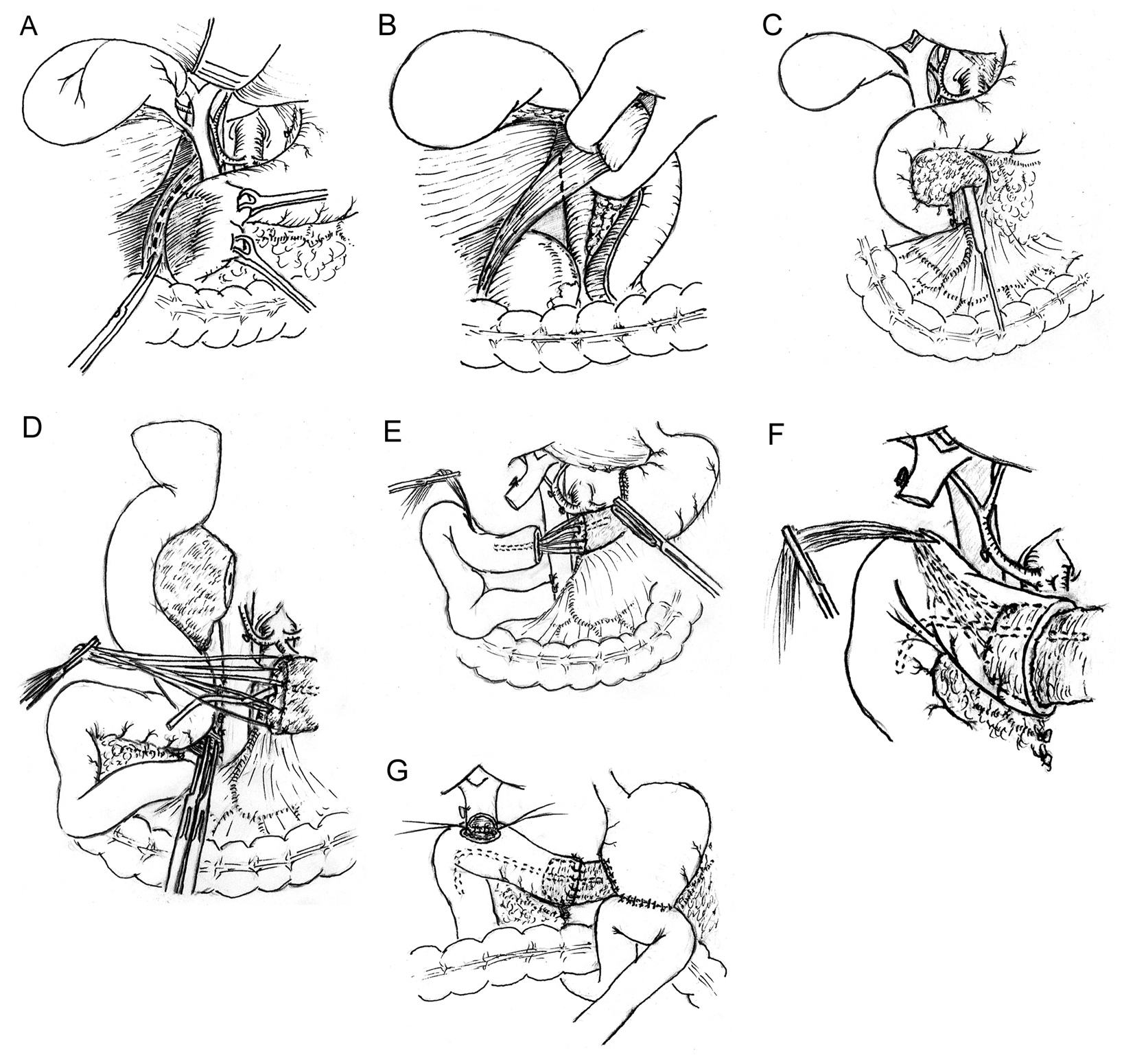
Figure 1. Modified pancreaticoduodenectomy with pancreaticojejunostomy by direct invagination of the pancreas into the jejunum that is brought up via the space behind the root of superior mesenteric vessel. (A, B) A Kocher maneuver is performed by incising the peritoneum lateral to the duodenum; the duodenum and the head of pancreas are reflected to the opposite direction; an inspection is carried out to detect if infiltration and adhesion of the tumor of pancreatic head to the inferior vena cava exists. (C) Using maxillary sinus stripper to explore evidence of infiltration and adhesion of tumor to the superior mesenteric vein (SMV), especially the uncinate tumor invasion of the right lateral surface and the undersurface of the SMV, to assess the resectability of the tumor. (D) All the sutures placed at the transected edges of the pancreas were left uncut to be used to pull the pancreas remnant into the jejunal lumen. The remnant pancreas was dissected free for 3 cm to ensure an invaginated anastomosis. The uncinate process of pancreas and the third and fourth portions of the duodenum were divided, leaving the jejunum intact. The upper jejunum was mobilized after division of the ligament of Treitz and was then brought up through the space behind the root of superior mesenteric vessels to the region of pancreatic head and duodenum. The jejunum is transected approximately 10 cm from its beginning. (E, F) The end of the divided jejunum was drawn up to the pancreas remnant. A 1.5 cm enterotomy approximately 13 cm to the end of the transected jejunum is made on the antimesenteric surface of the jejunum with electrotome. A large curved clamp is passed through the enterotomy and the sutures placed at the cut end of the pancreas are grasped and pulled out of the enterotomy. Through pulling the sutures, the cut end of the pancreas is then invaginated 3 cm into the jejunal lumen; (G) Discontinuous sutures are placed circumferentially between the pancreas and the cut edge of the jejunum to complete the anastomosis.