Figures
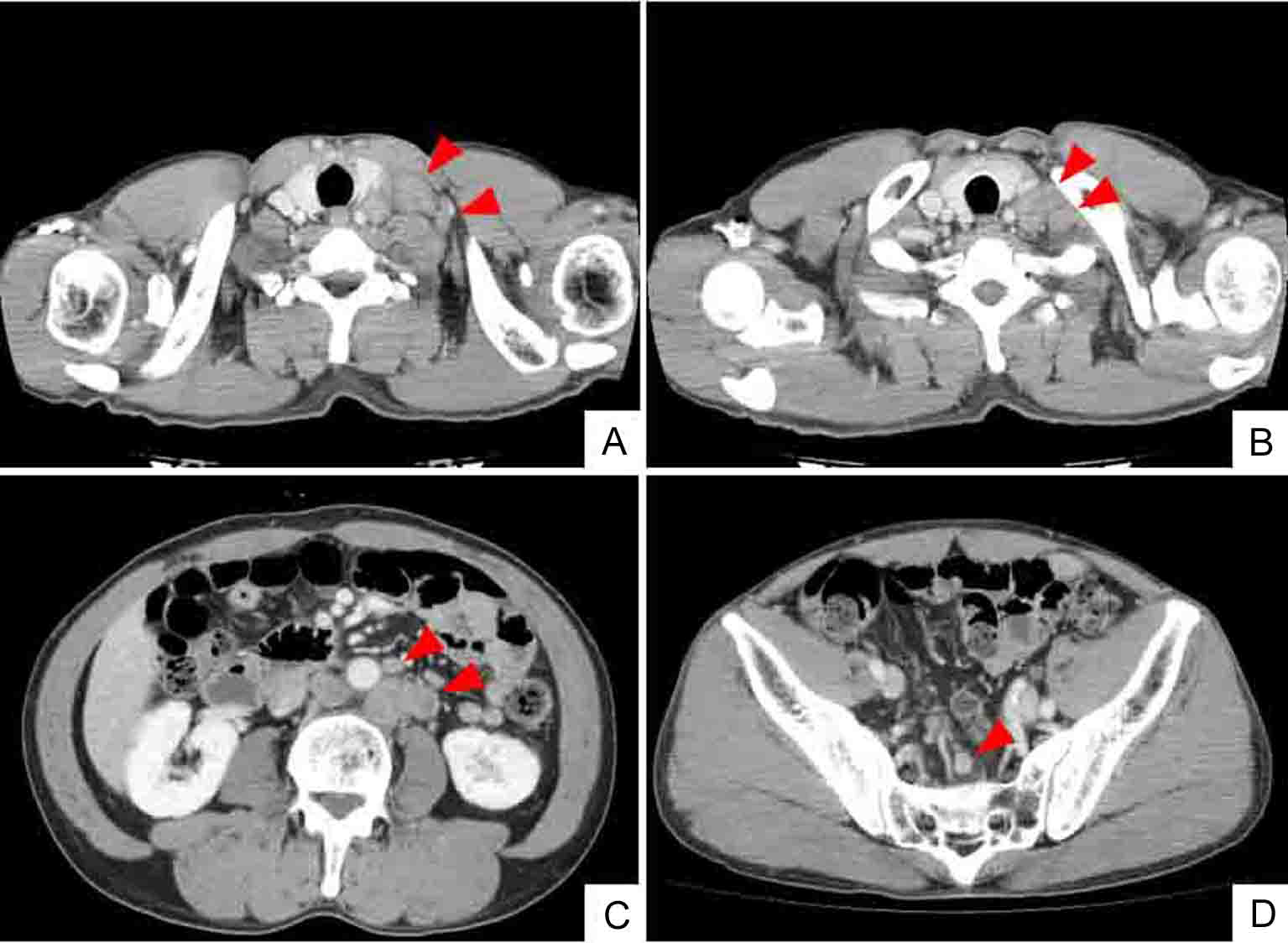
Figure 1. Whole body CT (computed tomography) shows mass of swollen left cervical (A) and supraclavicular (B) LNs. CT findings also indicate enlarged abdominal periaortic, inferior mesenteric and surrounding (C), and colic (D) LNs (arrowheads). However, CT findings do not indicate sigmoid colon tumor.
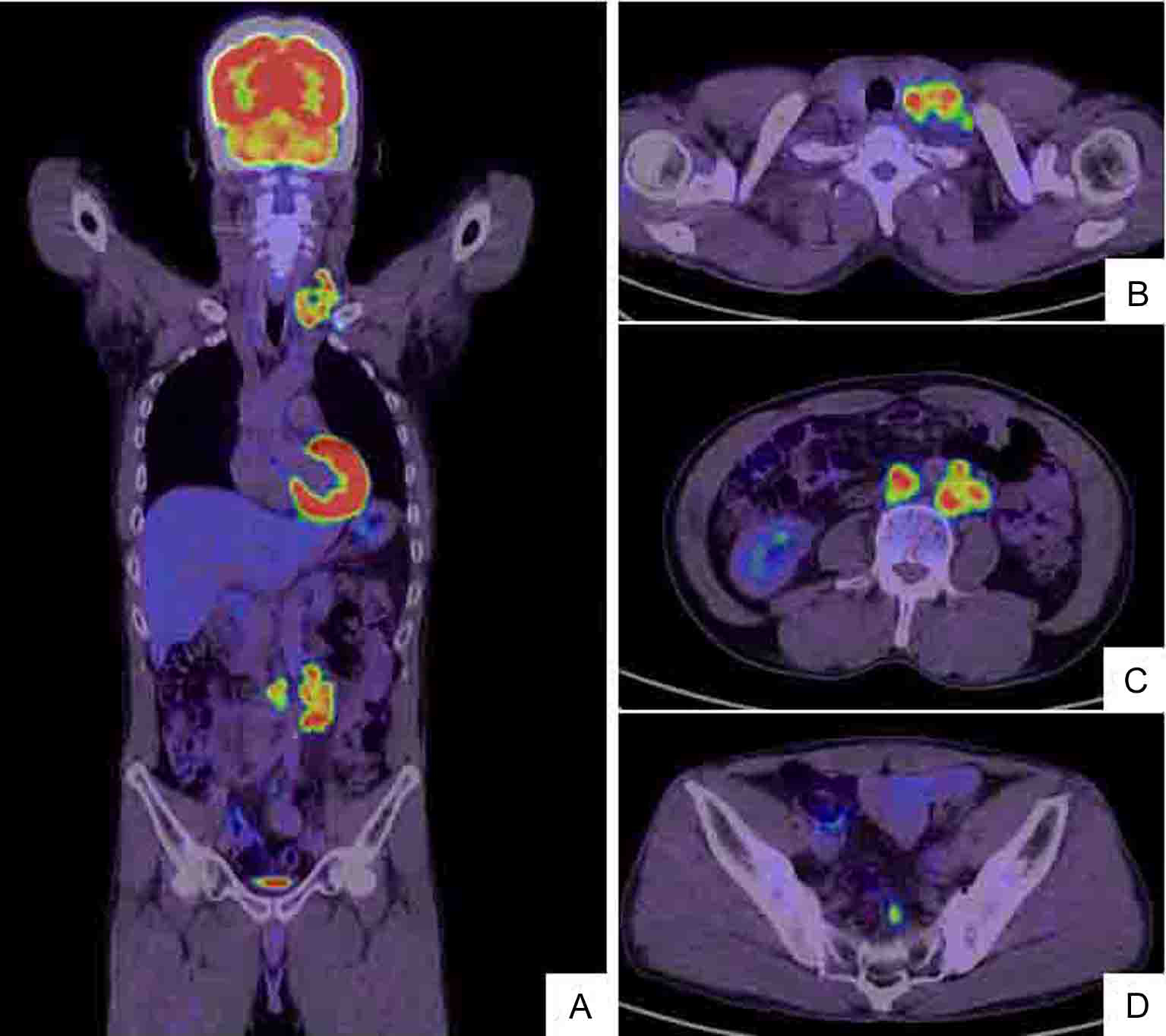
Figure 2. Whole body positron emission tomography (PET)/CT scan (A) shows hot lesions of multiple LN metastases to left cervix and left supraclavicular fossa (B) as well as enlarged left abdominal periaortic, inferior mesenteric and surrounding (C) and colic (D) LNs. The PET/CT and CT findings are identical (Fig. 1).
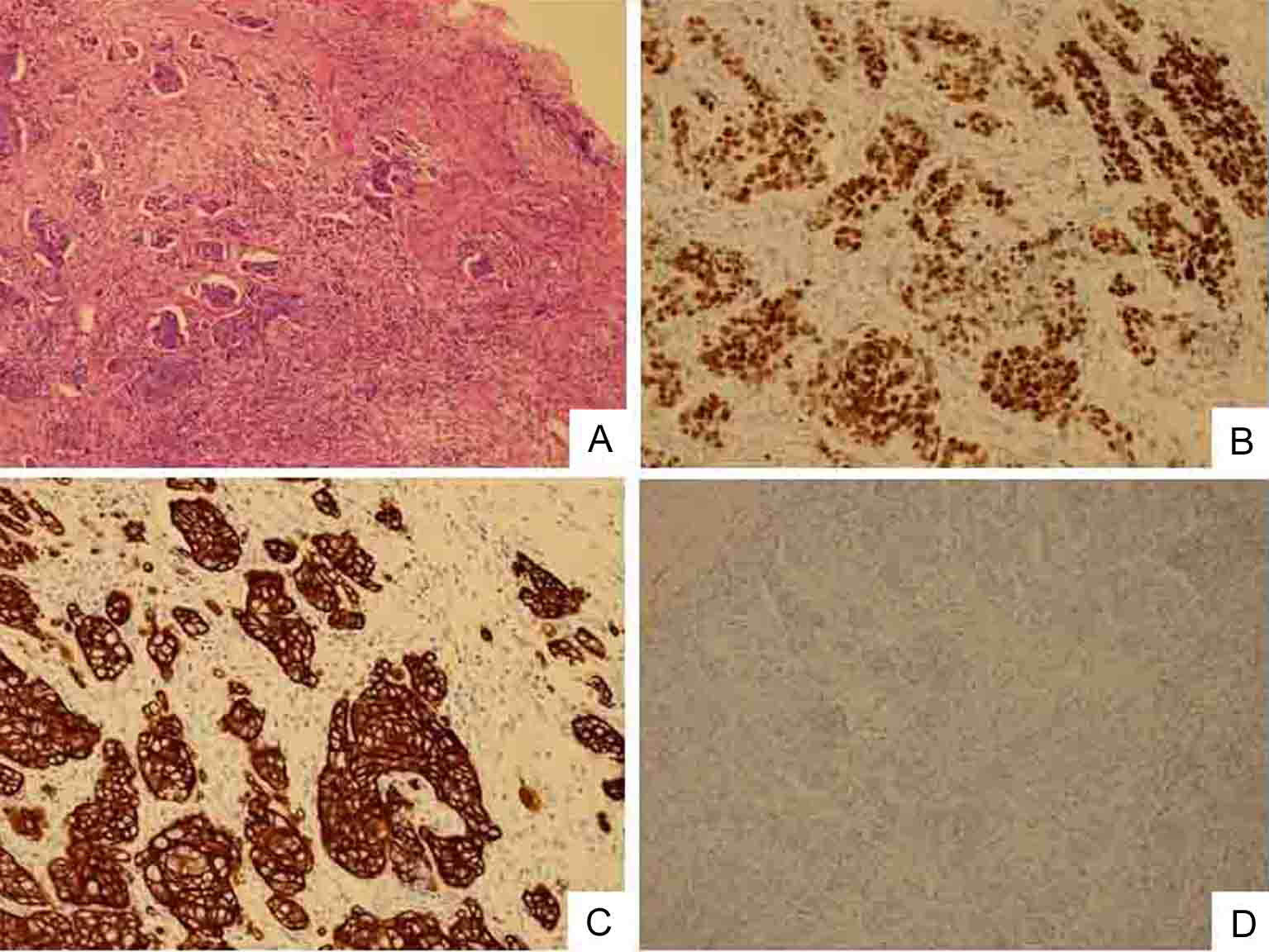
Figure 3. Biopsy specimen of swollen left clavicular LN. Cells are poorly differentiated adenocarcinoma. (A) HE staining (original magnification, × 100). Immunostaining shows that cancerous cells have nuclear expression of Cdx2 protein (B), intense and widespread positivity for CK20 protein (C) and negative immunostaining for CK7 (D).
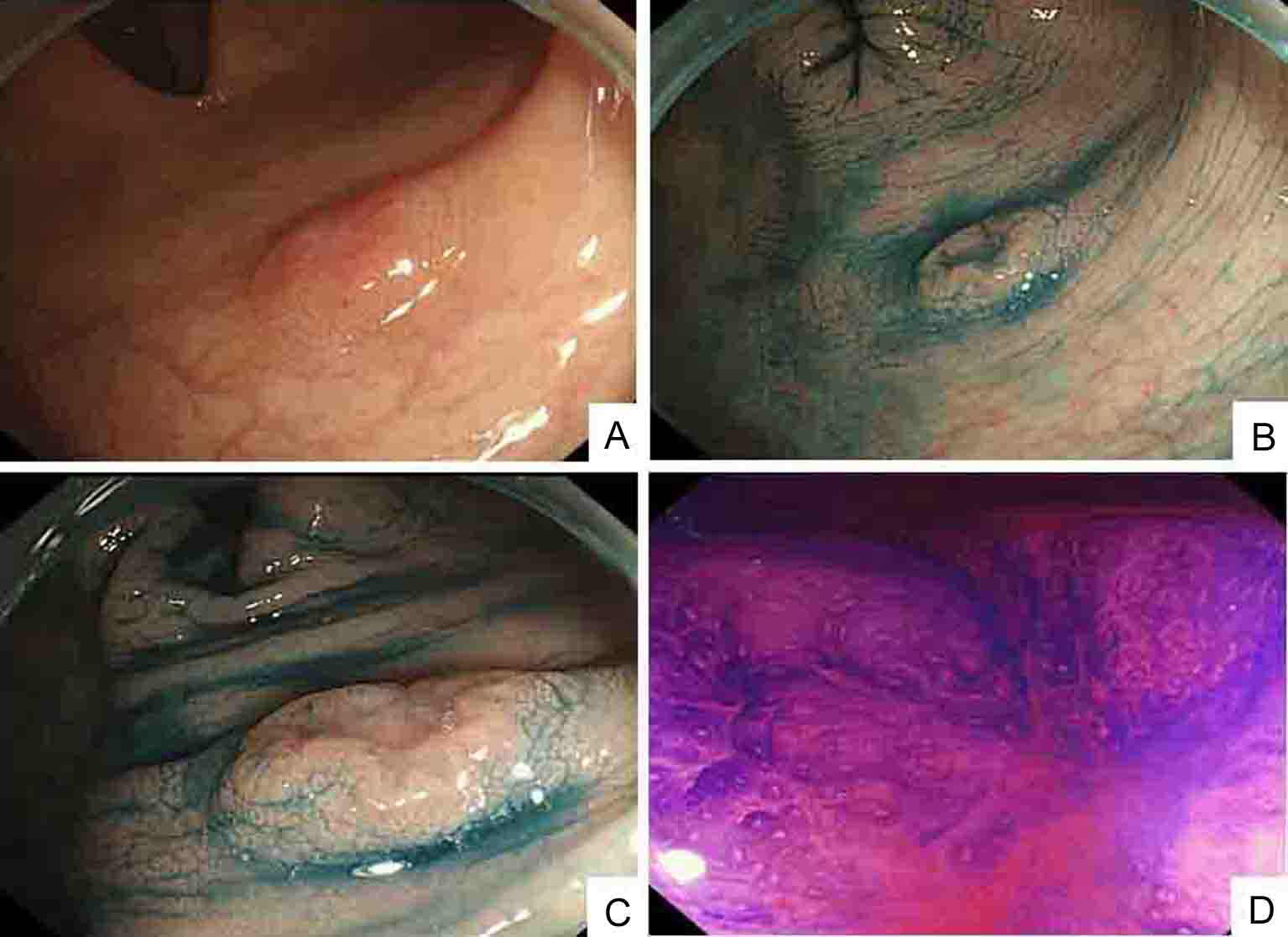
Figure 4. Colonoscopic findings: (A); indigo carmine contrast spray (B and C) demonstrate depressed type lesion 10 mm in diameter with distinct margins and marginal elevation (IIa+IIc type); crystal violet contrast spray (D) reveals pit pattern in central portion of tumor indicating VI type.
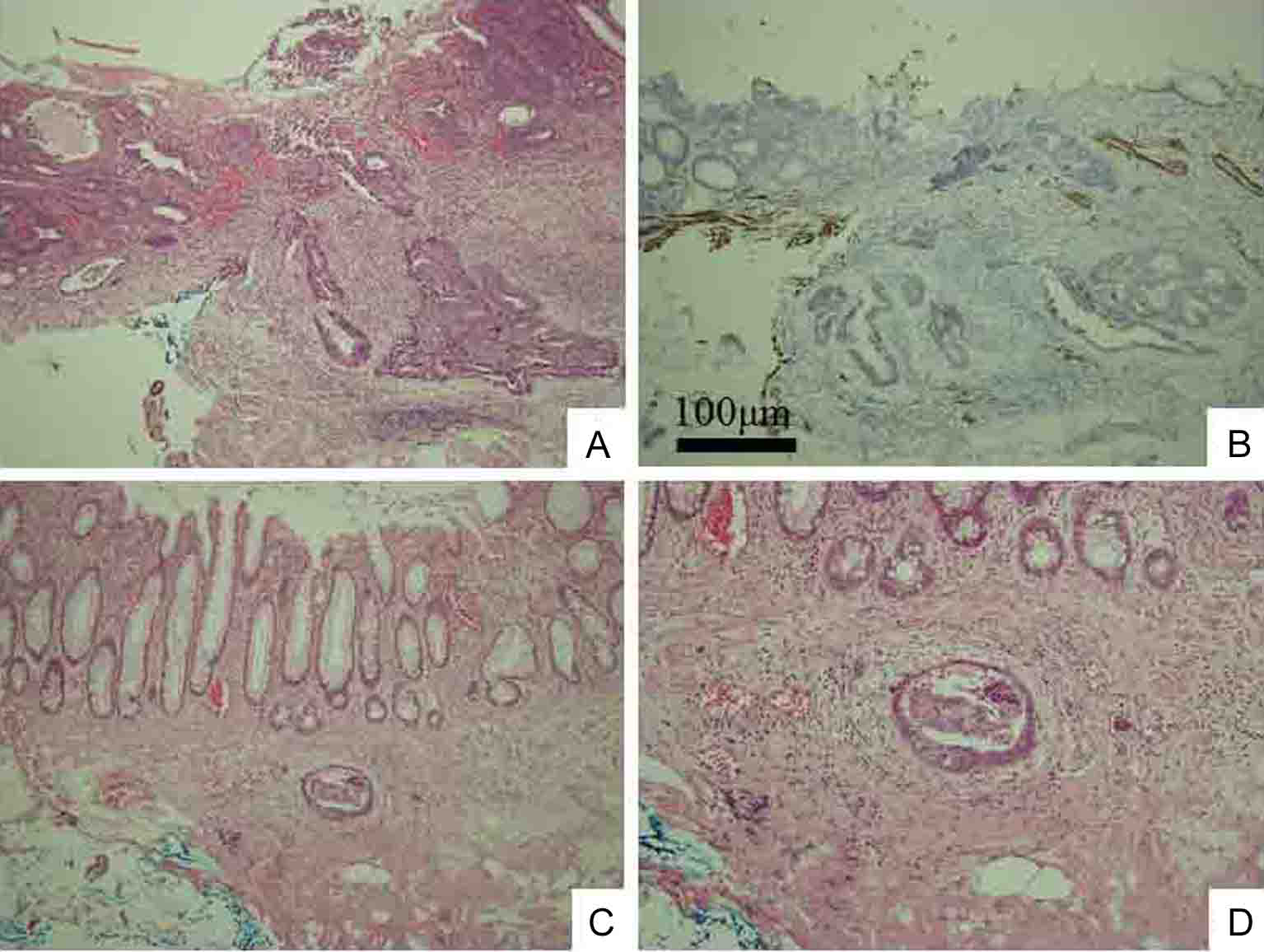
Figure 5. Histological examination shows moderately and poorly differentiated adenocarcinoma without adenoma component, indicating de novo development (A). Immunohistochemistry of desmin shows cancerous invasion of shallow SM to 450 µm from muscular layer of mucosa (B). Lymphovascular permeation of peritumoral submucosal lymphatics (C). Higher magnification of C (D). Original magnification: A, B, and C × 100; D × 200.
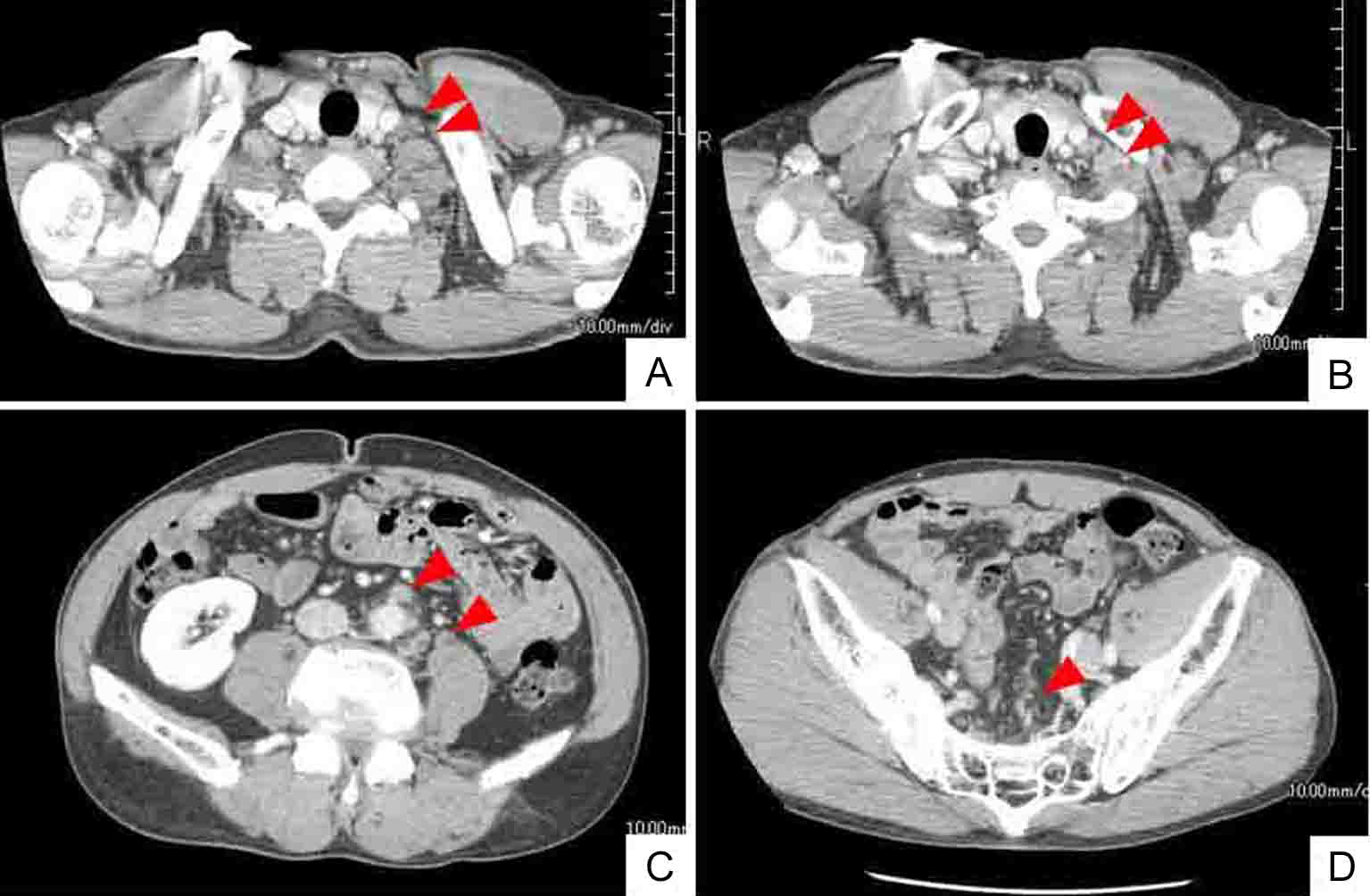
Figure 6. Whole body CT after 6 courses of chemotherapy (mFOLFOX6 and bevacizumab) shows smaller or disappeared metastatic LNs (arrow heads). Left cervical (A) and left supraclavicular (B) LNs. Abdominal periaortic, inferior mesenteric and surrounding (C), and regional colic (D) LNs.
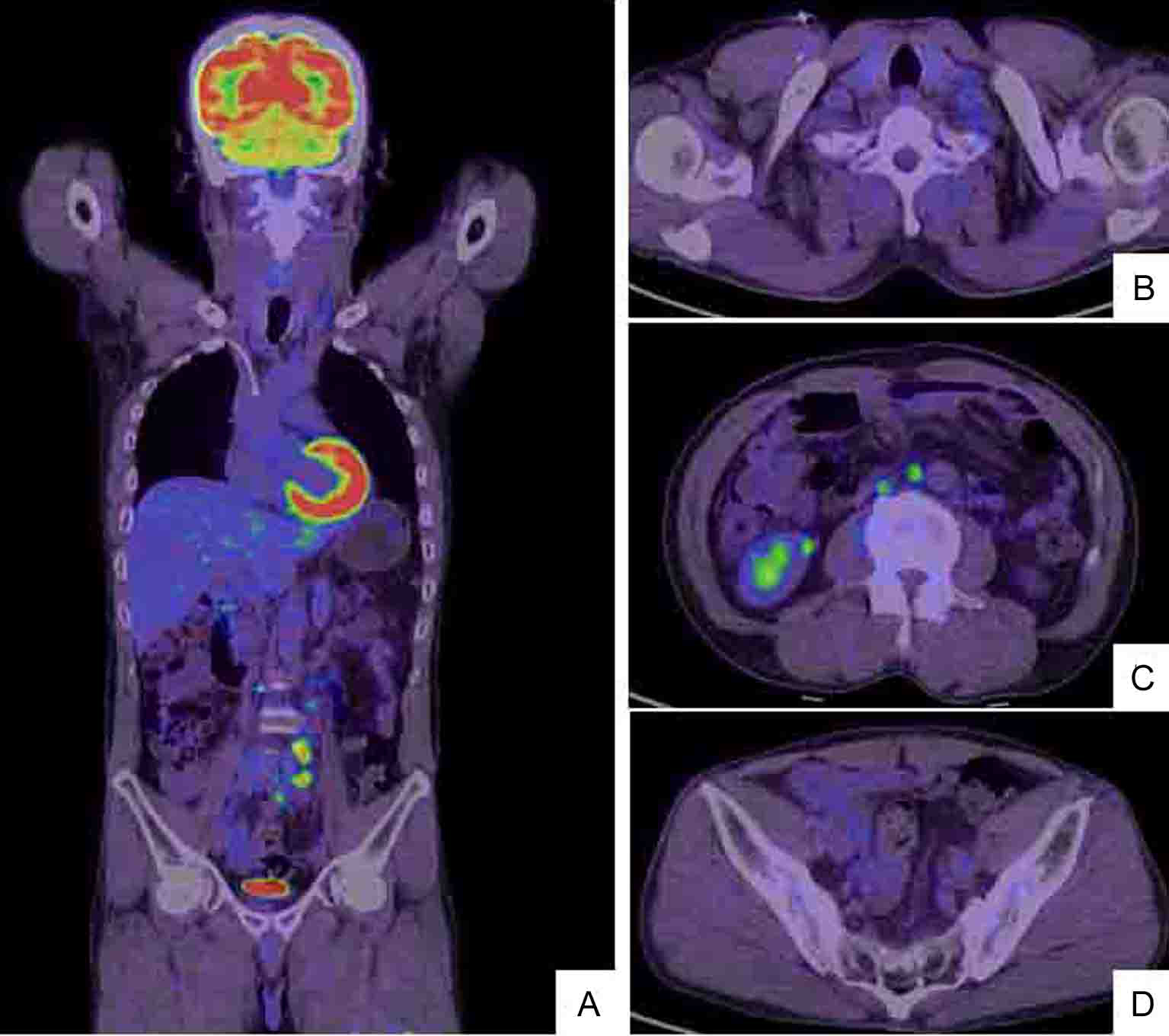
Figure 7. After 6 courses of the chemotherapy (the combination of mFOLFOX6 and bevacizumab), whole body PET/CT scan (A) demonstrates that the left cervical metastatic LNs (B) and the abdominal periaortic LNs are reduced in size and the intensity of hot lesions is obviously decreased (C). The regional colic LNs (D) are not recognized as hot lesions.