| Portal tract changes | |
| P1: Portal inflammation | Presence of mononuclear cells with or without interface activitya |
| P2: Bile ductular proliferation | Multiple bile ductules in a portal tracta |
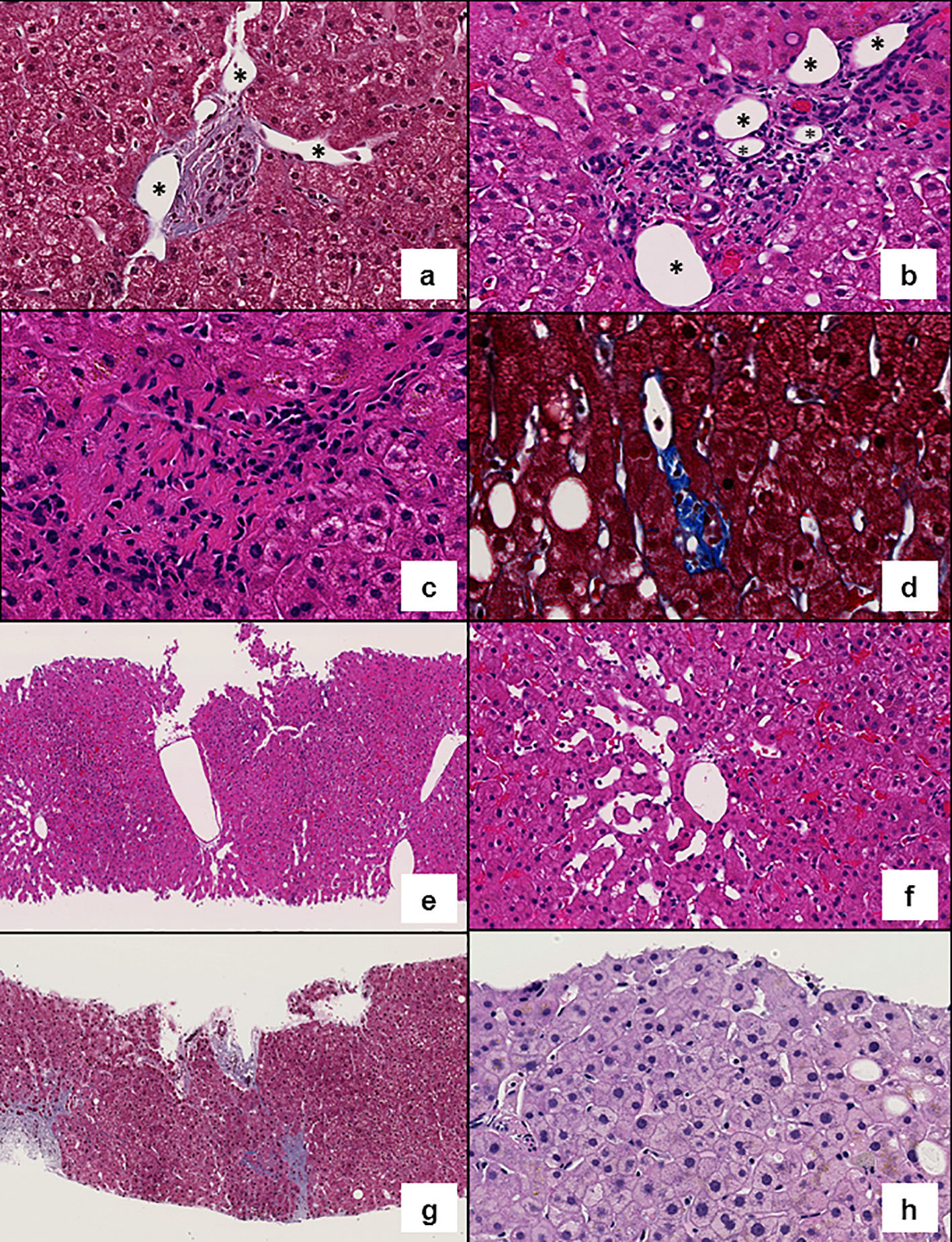
| P3: Shunt vessel (periportal) | Portal venous branches communicating with and herniating into the surrounding liver parenchymaa |
| P4: Increased number of portal vessels | Multiple portal vein branches in a portal tracta |
| P5: Obliterative portal venopathy | Phlebosclerosis; partial or complete obliteration of the portal venous lumena |
| P6: Rudimentary portal tract | Hypoplastic portal tract in which the lumen of the bile duct is smaller than the diameter of the surrounding hepatocytesa |
| Lobular changes | |
| L1: Central vein clustering | Increased central veins per lobule, arbitrarily defined as four or more CVs per lobule at medium (× 10) magnificationa |
| L2: Sinusoidal dilatation | Dilated sinusoidsa |
| L3: Iron granularity | The magnifications at which the granules are seen (naked eye, × 2, × 4, × 10, × 20, × 40) |
| L4: Iron zonation | Localization of iron granules: zone 1, zone 2 or zone 3 |
| L5: Incomplete septa | Thin fibrous septum arising from a portal tract blindly ending in the lobulea |
| L6: Perisinusoidal fibrosis | Fibrosis of zone 3 sinusoidsa |
| L7: Fibrosis | METAVIR fibrosis stage: F1, F2, F3, F4 |
| L8: Anisocytosis | Size variation in hepatocytes as a surrogate for nodular regenerationa |
| Total number of portal tracts in the sample | |
| Features of fatty liver disease (> 5% of steatosis and ballooning degeneration) | |