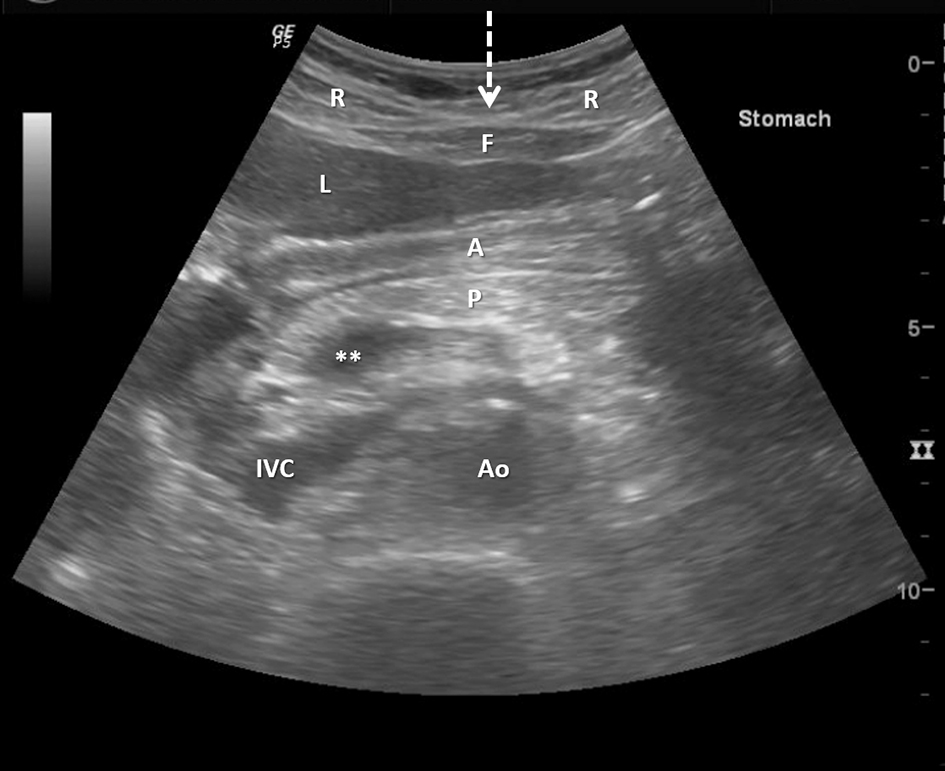
Figure 1. Pre-procedure ultrasound is performed in order to identify the margins of the liver and the location of the stomach and surrounding structures. R: rectus abdominis muscle; F: midline sub-rectus fat pad (arrow demonstrating midline linea alba); L: liver; A: antrum of stomach; P: pancreatic body; IVC: inferior vena cava; Ao: Aorta. **Portal confluence. The pre-procedure abdominal ultrasound is performed prior to stomach insufflation (which may or may not move the liver margin and allow for access through the linea alba).
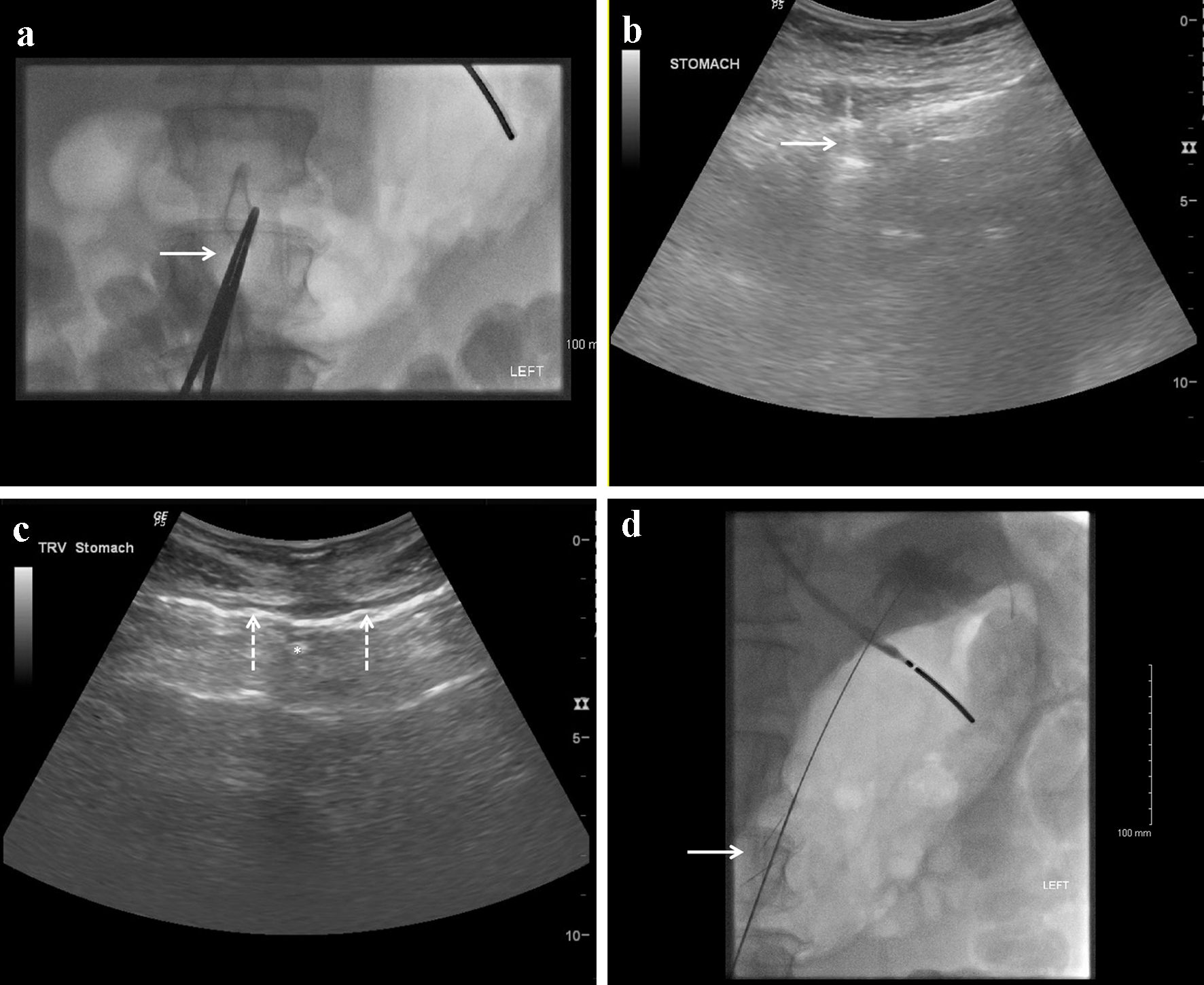
Figure 2. (a) Fluoroscopic image of the stomach insufflated with carbon dioxide with a superimposed clamp (arrow) on the patient’s skin surface to mark the area for ultrasound guided antral access (note the distal end of the enteric tube seen in the fundus of the stomach). (b) Ultrasound guided placement of gastropexy through the rectus abdominal muscle lateral to the linea alba. (c) Ultrasound guided gastric access with an 18-gauge needle through the linea alba. *Gastric access needle tip. Gastropexy anchors anchoring the stomach to the anterior abdominal wall are denoted by arrows on both sides of the access needle. (d) Fluoroscopic image demonstrating a stiff guide wire through the access needle in between the gastropexy suture anchors (arrow) angled towards the fundus.