










| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Case Report
Volume 10, Number 6, December 2017, pages 369-371
Transient Adult Jejunojejunal Intussusception: A Case of Conservative Management vs. Surgery
Jonathan Laia, c, Daryl Ramaia, Tyler Murphya, Fanny Kasherb
aDepartment of Anatomical Sciences, School of Medicine, St. George’s University, True Blue, Grenada, WI
bDepartment of Surgery, Richmond University Medical Center, Staten Island, NY, USA
cCorresponding Author: Jonathan Lai, Department of Anatomical Sciences, School of Medicine, St. George’s University, True Blue, Grenada, WI
Manuscript submitted June 29, 2017, accepted September 5, 2017
Short title: Transient Adult Intussusception
doi: https://doi.org/10.14740/gr881w
| Abstract | ▴Top |
Transient intussusception without any underlying lead is a rare clinical entity which can cause abdominal pain in adults. It has been associated with inflammatory bowel disease, cystic fibrosis, and endocrinological disorders. We present a case of transient jejunojejunal intussusception in a 42-year-old Hispanic male patient without any underlying pathological lead point. Surgical intervention yielded a negative laparotomy and resection was not undertaken. We discuss the clinical presentation, surgical procedure, risk factors leading to episodes of transient intussusception, and the use of surgery versus conservative management in such cases.
Keywords: Adult intussusception; Laparotomy; Transient intussusception
| Introduction | ▴Top |
Intussusception is a rare cause of abdominal pain in adults, and accounts for 1-5% of mechanical bowel obstructions [1]. Telescoping of the bowel, most commonly at the ileocecal junction, leads to bowel obstruction which presents with bloody and mucoid loose stools. In adults, most cases are the result of intestinal pathology, which makes transient intussusception without any pathological connection a very rare clinical entity. We present a case of transient intussusception in a patient without any underlying lead point.
| Case Report | ▴Top |
A 42-year-old Hispanic male with a history of diabetes presented with severe intermittent lower left quadrant pain 3 - 4 times a day. He denied having this pain in the past, nor associated nausea, vomiting, and change in appetite. A palpable soft and non-tender mass was palpable on his abdomen; otherwise the abdomen was soft, non-tender, non-distended, with mild voluntary guarding on the left lower quadrant. There was no rebound tenderness, or signs suggestive of peritonitis. Digital rectal exam showed no rectal masses, hemorrhoids, nor gross blood, and stool guaiac test was negative. His glucose levels were well controlled, and liver enzymes and electrolytes were within normal limits.
The patient was hemodynamically stable but under distress, which prompted a computed tomography (CT) scan of his abdomen and pelvis which revealed telescoping of the small bowel (Fig. 1), and a “target sign” appearance (Fig. 2) which suggested intussusception. A nasogastric (NG) tube was placed and planned for conservative management. However, due to exacerbating abdominal pain, he was scheduled for surgery the next day. A vertical midline incision allowed evisceration of the bowel. Running the bowels twice from the ileocecal valve until the ligament of Treitz showed no evidence of intussusception, lead point, inflammation, or ischemia.
 Click for large image | Figure 1. Sagittal image of a contrast-enhanced CT scan of the abdomen. The mesentery is seen to twist as bowel begins to telescope through another loop of bowel (red circle). |
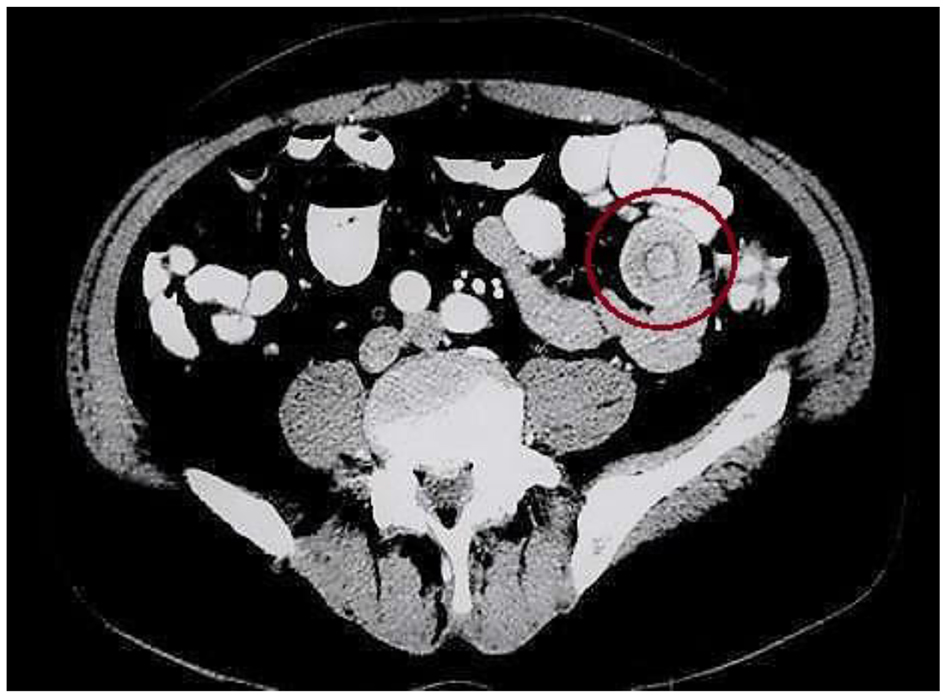 Click for large image | Figure 2. The characteristic “target sign” appearance of intussusception can be appreciated (red circle). |
During post-operative evaluation, our patient reported significant improvement of abdominal pain. The NG tube was removed and was discharged on post-operative day 3 after tolerating solid food, and flatulent with bowel movements. He was instructed to follow up with his general practitioner for routine check-ups and screening.
| Discussion | ▴Top |
While most cases of transient intussusception are idiopathic, it has been reported in adults with celiac and Crohn’s disease [2]. It is believed that in these malabsorption syndromes, the dilated flaccid loops of bowel undergo hypersecretion which disturbs natural peristalsis and leads to telescoping of the bowel walls [3]. Interestingly, endocrinological complications secondary to hyperglycemia, metabolic acidosis, and hyperkalemia have been associated with intestinal dysmotility and intussusception [4, 5]. However, due to a lack of published reports, it is unclear whether correction of metabolic derangements results in spontaneous reduction. Furthermore, Artul et al (2013) reported a self-resolving case of intussusception in a cystic fibrosis patient. Kehagias et al (2009) reported intussusception as the initial clinical sign of human immunodeficiency virus (HIV) infection [6, 7].
With the increasing use of imaging techniques and the overutilization of CT scans, idiopathic and asymptomatic intussusception may be diagnosed more often. In cases where intussusception is associated with a pathologic entity and signs of bowel obstruction or GI bleeding, exploratory laparotomy should be performed. In contrast, other cases of small bowel intussusception may have a benign or clinical course as described above. In these cases, the use of explorative surgery has been debated. However, laparoscopy with reduction has become an acceptable strategy to aid in decision making, surgical planning, and treatment as well. In our case, initial conservative management did not yield any improvement in the patient’s condition, and due to his escalating presentation, surgery was planned to milk out the intussuscepted bowels and evaluate for possible malignancy.
While surgery is often employed when intussusception is associated with an underlying pathological lead point, its use in cases of transient cases is questionable. It has been observed that in cases of intussusception where the length of involvement is less than 3.5 cm, it tends to be self-resolving [8]. In these cases, intussusception resolves without any specific treatment [1]. Patients should undergo conservative management with appropriate with bowel rest, IV fluids, labs, and follow-up imaging studies to monitor the resolution status of intussusception. This avoids costly and time consuming surgical interventions. Alternatively, small bowel enteroscopy or capsule endoscopy can be used if not obstructed to screen for luminal lesions that may lead to intussusception. However, caution should be taken when interpreting these results as luminal lesions can be mistaken for other diseases. Giestas et al (2016) reported a case of intussusception with a false negative capsule endoscopy where a gastrointestinal stromal tumor (GIST) was mistaken for angiodysplasia [9].
In conclusion, adult intussusception is a very rare clinical entity and should be meticulously investigated for underlying pathology. We report a case of jejunojejunal intussusception which leads to surgical intervention. However, this leads to a negative laparotomy and no resection was undertaken. Although this yielded a negative laparotomy, further research is needed to shed light on how long conservative management should be allowed, or when would surgery be considered in patients with no significant medical history.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.
Consent
Informed consent was obtained.
| References | ▴Top |
- Marinis A, Yiallourou A, Samanides L, Dafnios N, Anastasopoulos G, Vassiliou I, Theodosopoulos T. Intussusception of the bowel in adults: a review. World J Gastroenterol. 2009;15(4):407-411.
doi pubmed - Napora TE, Henry KE, Lovett TJ, Beeson MS. Transient adult jejunal intussusception. J Emerg Med. 2003;24(4):395-400.
doi - Catalano O. Transient small bowel intussusception: CT findings in adults. Br J Radiol. 1997;70(836):805-808.
doi pubmed - Koh JS, Hahm JR, Jung JH, Jung TS, Rhyu SS, Moon SW, Kang MY, et al. Intussusception in a young female with Vibrio gastroenteritis and diabetic ketoacidosis. Intern Med. 2007;46(4):171-173.
doi pubmed - McFarlane SI, Byrne K, Shin J, Williams R. Intussusception in an adult patient with severe hyperglycaemia--a case report. Diabet Med. 2002;19(7):611-614.
doi pubmed - Artul S, Artoul F, Habib G, Abboud N. Transient intussusception: rare cause of abdominal pain in cystic fibrosis. BMJ Case Rep. 2013;2013.
- Kehagias I, Karamanakos SN, Panagiotopoulos S, Giali S, Gogos CA, Kalfarentzos F. A rare case of intussusception leading to the diagnosis of acquired immune deficiency syndrome: a case report. J Med Case Rep. 2009;3:61.
doi pubmed - Lvoff N, Breiman RS, Coakley FV, Lu Y, Warren RS. Distinguishing features of self-limiting adult small-bowel intussusception identified at CT. Radiology. 2003;227(1):68-72.
doi pubmed - Giestas S, Almeida N, Martins R, Canhoto A, Oliveira P, Figueiredo P, Sofia C. Small Bowel GIST: Clinical Presentation as Intussusception and Obscure Bleeding. GE Port J Gastroenterol. 2016;23(5):279-281.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.