

| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Original Article
Volume 10, Number 2, April 2017, pages 78-83
Correlation Between Symptom Severity and Health-Related Life Quality of a Population With Gastroesophageal Reflux Disease
Shou-Wu Leea, b, d, Teng-Yu Leea, b, Han-Chung Liena, c, Yen-Chun Penga, c, Hong-Jeh Yeha, c, Chi-Sen Changa, b
aDivision of Gastroenterology and Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan, Republic of China
bDepartment of Internal Medicine, Chung Shan Medical University, Taichung, Taiwan, Republic of China
cDepartment of Internal Medicine, Yang-Ming University School of Medicine, Taipei, Taiwan, Republic of China
dCorresponding Author: Shou-Wu Lee, Division of Gastroenterology, Department of Internal Medicine, Taichung Veterans General Hospital, No. 160, Sec. 3, Chung-Kang Road, Taichung 407, Taiwan, Republic of China
Manuscript accepted for publication March 14, 2017
Short title: Symptom Severity and Life Quality in GERD
doi: https://doi.org/10.14740/gr753w
| Abstract | ▴Top |
Background: Gastroesophageal reflux disease (GERD) is a chronic disease with a negative impact on the quality of life. The aim of this study was to investigate the reflux symptoms and the health-related quality of life in a population with GERD.
Methods: Data from patients with GERD, according to the Montreal definition, were collected between January and December 2009. The enrolled patients were classified by different reflux symptoms according to the modified Chinese GERDQ. The general demographic data, the modified GERD impact scores and the SF-36 questionnaire scores of these groups of patients were analyzed.
Results: A total of 173 patients were enrolled, and the general data, endoscopic findings and lifestyle habits of the participants with different severity of heartburn or regurgitation were all similar. The patients with moderate severity of reflux symptoms had significant lower SF-36 scores than those with mild severity. The cases with advanced heartburn severity owned the lowest scores among all cases. The impact on the daily activity of each affected individual had a positive association with the stronger severity of reflux symptom.
Conclusion: The life quality of a population with GERD achieved the meaningful declination in participants with the moderate severity of heartburn or regurgitation. The severity of the reflux symptoms had a greater impact on the normal daily activity of the patients with GERD. The cases with advanced severity of heartburn had the worst well-being.
Keywords: Erosive esophagitis; Gastroesophageal reflux disease; Gender; Life’s quality; Non-erosive reflux disease
| Introduction | ▴Top |
Gastroesophageal reflux disease (GERD) is a chronic disease that tends to relapse and develop complications. According to the Montreal definition, GERD is defined as “a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications” [1]. Heartburn and regurgitation are the typical symptoms of GERD, but patients with the disease may also have other symptoms, such as epigastric pain and sleep disturbance. As per Genval guidelines, a negative impact on the quality of life is stated as a criterion for reflux disease in patients with frequent heartburn [2]. Moreover, GERD has an impact on the everyday lives of affected individuals, and interferes with physical activity, impairs social functioning, disturbs sleep and reduces productivity at work [3-6]. The evaluation of patient-based quality of life as a medical care outcome is generally confined to health-related quality of life (HRQoL). HRQoL is lower in individuals with GERD than in the general population, and is comparable to that in individuals with other chronic diseases, such as diabetes, arthritis or chronic heart failure [3]. There are two categories of HRQoL measures: disease-specific and generic HRQoL instruments. Disease-specific instruments are used to describe the burden of disease and treatment outcomes in patients with a specific disease, and generic instruments measure the overall HRQoL of patients, including physical, emotional, and social function, as well as their level of general performance at work and in daily life across different diseases. The aim of this study was to investigate the reflux symptoms and the HRQoL in a Chinese population with GERD.
| Methods | ▴Top |
Data from consecutive patients with GERD in our hospital, diagnosed by the Montreal definition, were collected from January 2009 to December 2009. Exclusion criteria were as follows: 1) GERD combined with other structural gastrointestinal disorders, such as peptic ulcer disease, esophageal or gastric malignancy; 2) prior gastric surgery; 3) use of chronic anti-acid medication, such as proton pump inhibitors (PPIs) or H2-receptor antagonists (H2RAs), for more than 2 months prior to enrollment; and 4) pregnancy.
The general data of enrolled patients, including age, gender, body weight, body mass index (BMI), symptom duration and lifestyle habits, were recorded. All patients underwent an open-access transoral upper gastrointestinal endoscopy, and the findings of esophagocardiac mucosal break, ulcer, hiatal hernia or Helicobacter pylori infection of each case were collected. All cases had been asked to complete the questionnaires, including the modified Chinese GERDQ, the modified GERD impact scale, and the SF-36 questionnaire (Chinese version).
The modified Chinese GERDQ was included with the severity of the symptoms of regurgitation and heartburn, graded on a three-point Likert scale. Mild, moderate and advanced severity were defined as symptoms which can be easily ignored, awareness of symptoms but easily tolerated, and symptoms sufficient to cause an interference with normal activities, respectively. The modified GERD impact scale measured the frequency of imparied daily activity, including sleep interruption, eating or drinking problem, and word interferences, graded on a three-point Likert scale: never, sometimes and daily.
The SF-36 questionnaire measured generic quality of life, which allowed comparisons between different disease states. It measured health status in eight domains: physical functioning, role limitations - physical, bodily pain, general health, vitality, social functioning, role limitations - emotional, and mental health. Two summary scores were also calculated from subject responses: the physical health (PH) score and the mental health (MH) score. Scores on the SF-36 ranged from 0 to 100 on each dimension and on the summary scales, with higher scores indicating better quality of life.
Data were expressed as standard deviation of mean for each of the measured parameters. Gender, hiatal hernia, lifestyle habits, the modified Chinese GERDQ items and the modified GERD impact scale, were expressed as a percentage of the total patient number. A P value below 0.05 was considered statistically significant. Pearson’s Chi-square test or Fisher’s test was used to compare the effects of gender, hiatal hernia, lifestyle habits and the modified Chinese GERDQ and the modified GERD impact scale scores; ANOVA test was used to analyze age, body weight, BMI, and scores of SF-36 questionnaires.
| Results | ▴Top |
A total of 173 consecutive patients were enrolled, as shown in Table 1. One hundred ten (63.6%), 54 (31.2%), and nine (5.2%) patients, and 81 (46.4%), 68 (39.3%), and 24 (13.9%) cases, had the mild, moderate and advaced severity of heartburn and regurgitation, measured by the modified Chinese GERDQ, respectively. The general data, endoscopic findings and lifestyle habits of the participants with different severity of heartburn or regurgitation were all similar in each item.
 Click to view | Table 1. Characteristics of the Enrolled Patients With GERD |
The total scores, PH scores and MH scores, measured by the SF-36 questionnaire, among patients of different severity of heartburn and regurgitation, are shown in Figs. 1 and 2, respectively. The patients with moderate severity of heartburn had significant lower scores than those with mild severity of symptom, no matter in the total health scores (57.15 ± 18.76 vs. 70.59 ± 14.85), PH scores (59.01 ± 18.79 vs. 69.64 ± 14.61), or MH scores (51.06 ± 18.25 vs. 65.51 ± 16.30). The significant difference still existed in the total scores, but not in the PH scores and MH scores, between the patients with advanced severity of heartburn (total mean scores: 48.56 ± 15.32, PH scores: 49.41 ± 21.76, MH scores: 46.01 ± 23.22) and those with moderate severity of symptom.
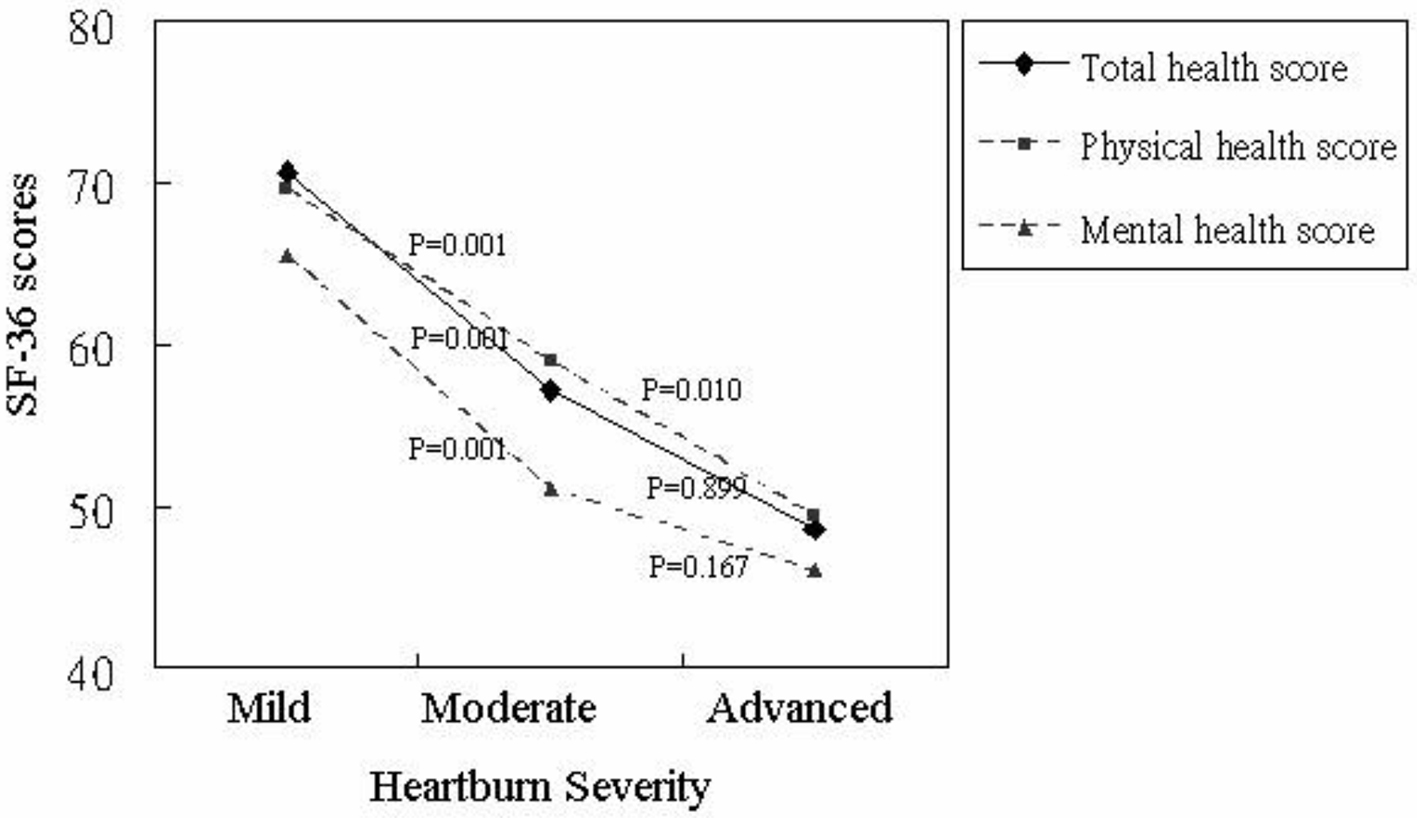 Click for large image | Figure 1. The results of the SF-36 questionnaire of patients with different severity of heartburn. |
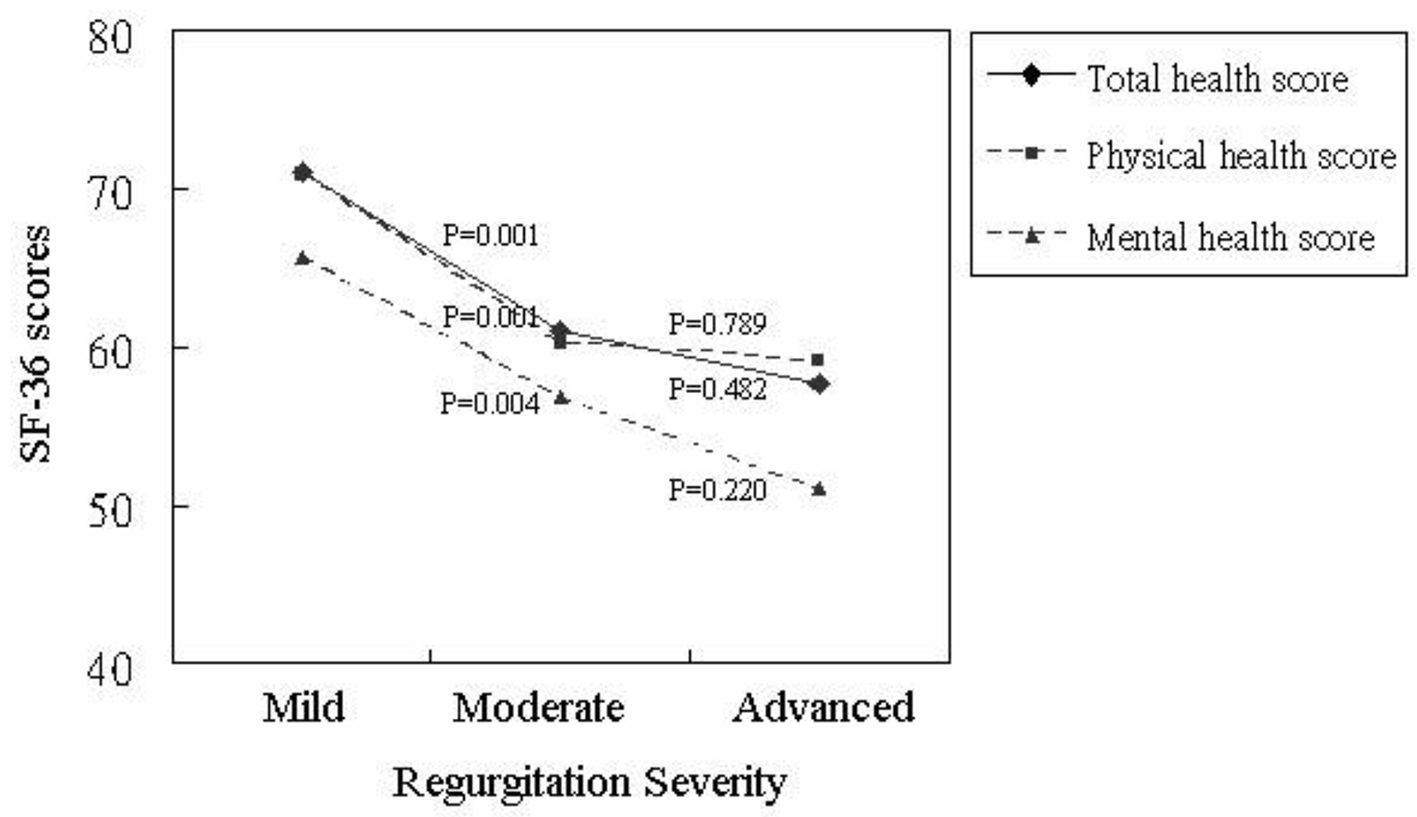 Click for large image | Figure 2. The results of the SF-36 questionnaire of patients with different severity of regurgitation. |
Similarly, the cases with moderate severity of regurgitation had significant lower scores than those with mild severity of symptom (total health scores: 61.03 ± 20.45 vs. 71.06 ± 13.25, PH scores: 60.25 ± 19.98 vs. 70.95 ± 12.79, MH scores: 56.81 ± 20.66 vs. 65.63 ± 15.01). There were no significant differences between the patients with advanced severity of regurgitation (total mean scores: 57.75 ± 16.69, PH scores: 59.04 ± 15.71, MH scores: 51.08 ± 15.58) and those with moderate severity of symptom.
The impact of symptoms of GERD on the daily activity of each affected individual, measured by the modified GERD impact scale, is summarized in Figs. 3 and 4. The frequency of sleep interruptions, eating or drinking problems, or work interferences, had a strongely positive association with the severity of heartburn and regurgitation.
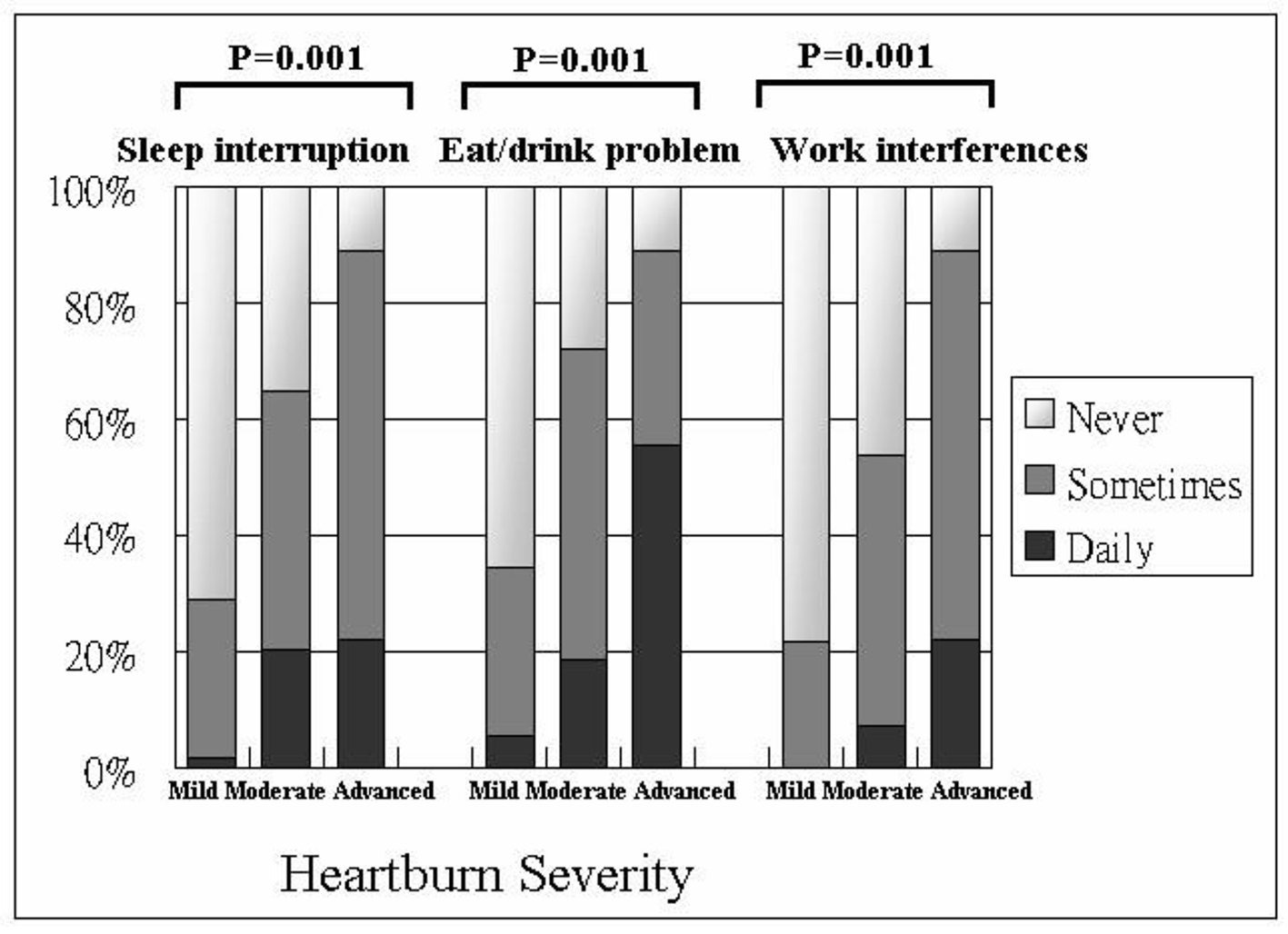 Click for large image | Figure 3. The results of the modified GERD impact scale of patients with different severity of heartburn. |
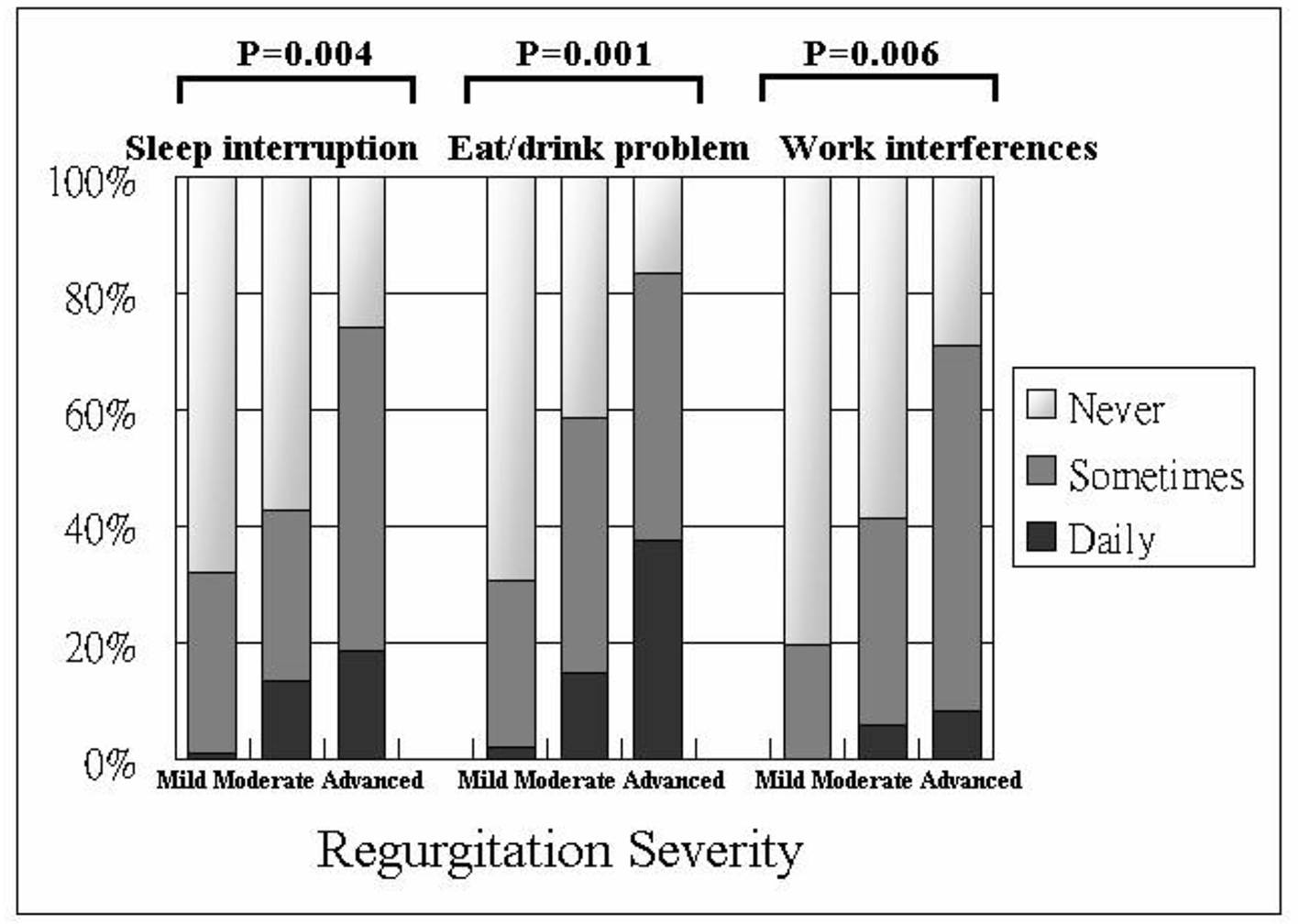 Click for large image | Figure 4. The results of the modified GERD impact scale of patients with different severity of regurgitation. |
| Discussion | ▴Top |
GERD is a chronic disease which has a considerable impact on the everyday lives of affected individuals, and interferes with physical activity, impairs social functioning, disturbs sleep and reduces productivity at work [3, 5, 6]. Symptoms associated with GERD include heartburn, acid regurgitation, and chest pain, as well as extraesophageal manifestations such as nausea, chronic cough, asthma, and hoarseness. All of these symptoms may compromise HRQoL. In addition, sleep disturbance and associated daytime sleepiness, decrease in mealtime enjoyment, and increased medication costs may contribute to the burden of disease [7].
The symptoms of GERD had a critical impact on HRQoL of these patients. Studies using validated instruments have shown that the presence of reflux symptoms is associated with impaired HRQoL in the general population in rural Sweden [8] and Australia [9]. One population-based study, including four reflux symptoms: heartburn, acid regurgitation, abdominal pain, and stomach pain, found an association of increasing symptom severity with a decrease in well-being. At least mild symptom of heartburn was associated with a clinically meaningful reduction in well-being [10]. Another study reported that weekly reflux symptoms were associated with meaningfully impaired HRQoL in the physical dimensions of SF-36, and daily symptoms had meaningfully impaired HRQoL in both physical and psychosocial dimensions [11]. In addition, greater symptom severity associated with significant decreases in well-being was confirmed in several previous studies [4, 12-16]. A recent systematic review of 19 studies, including a total of 55,834 participants with reflux symptoms, disclosed the mean PH and MH scores were 1.1 times lower in the groups with disruptive GERD than in those with non-disruptive GERD. The groups with more severe reflux symptoms had lower PH scores than those with less severe symptoms [17].
Similarly, our results provided significantly lower PH and MH scores in the patients with moderate severity of heartburn and regurgitation, compared to those with the mild severity of reflux symptoms. Interestingly and uniquely, the difference still existed between the groups with moderate and advanced severity of heartburn, but not in the groups with moderate and advanced severity of regurgitation. The reason may be due to the less case numbers with the advanced severity regurgitation symptoms, but this result also implies that moderate severity of reflux symptoms had achieved a dramatic reduction in HRQoL, and may warrant appropriate clinical management. Besides, the heartburn symptoms had a greater impact on HRQoL of affected individuals than the symptom of regurgitation did, and it may need more aggregative treatment.
The symptoms of GERD affect many aspects of patients’ lives, causing sleep disruption, less concentration and limitations in physical activity, as well as impairing psychosocial aspects of patient well-being, including enjoyment of social gatherings, intimacy and sex. Wahlqvist et al showed that patients with GERD symptoms report 23% reduced productivity while at work, and 30% reduced productivity while doing regular daily activities in a Swedish population [18]. Time absent from work for health reasons and reduction in productivity at work both became significantly more pronounced with increasing severity of GERD symptoms [4]. Data from other studies revealed a 6-10.7% decrease in work productivity in subjects with GERD [19-22].
Our study had a similar result, in which the daily activities, including sleep, drink or eat, and work, were disturbed by the symptom severity of heartburn and regurgitation. Furthermore, the more severe reflux symptoms there were, the more interruptions of normal daily activities they had.
There were some limitations in our study. Firstly, the HRQoL measures in our study, including the SF-36 questionnaire, the modified Chinese GERDQ, and the modified GERD impact scale, were all scored by the patients’ self-report, and a possibility of subject answers among different responders might be present. Secondly, co-morbidity diseases of these patients that tend to influence severity of GERD, such as chronic heart failure, chronic obstructive pulmonary disease, or overlapping inflammatory bowel disease, were not considered, and this might have led to inaccuracy of the data. Thirdly, the case number with the advanced severity or the high frequency of reflux symptoms was small in our study, and it may be the underlying reason for the lack of significant differences of each HRQoL measure compared to other cases. Lastly, our study’s design was hospital-based. Further researches in representative samples of the general population are needed to confirm these results.
Conclusion
In the present study, the patients with different severity of reflux symptoms had similar presentations of general characteristic, endoscopic findings or lifestyle habits. The generic HRQoL instruments revealed significant lower scores in GERD patients with moderate severity of reflux symptoms. The severity of the reflux symptoms also had a greater impact on the normal daily activity of the patients with GERD. The cases with advanced severity of heartburn had the worst well-being among all cases.
| References | ▴Top |
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101(8):1900-1920; quiz 1943.
- An evidence-based appraisal of reflux disease management - the Genval Workshop Report. Gut. 1999;44(Suppl 2):S1-16.
doi pubmed - Wiklund I. Review of the quality of life and burden of illness in gastroesophageal reflux disease. Dig Dis. 2004;22(2):108-114.
doi pubmed - Wahlqvist P, Karlsson M, Johnson D, Carlsson J, Bolge SC, Wallander MA. Relationship between symptom load of gastro-oesophageal reflux disease and health-related quality of life, work productivity, resource utilization and concomitant diseases: survey of a US cohort. Aliment Pharmacol Ther. 2008;27(10):960-970.
doi pubmed - Lee SW, Chang CM, Chang CS, Kao AW, Chou MC. Comparison of presentation and impact on quality of life of gastroesophageal reflux disease between young and old adults in a Chinese population. World J Gastroenterol. 2011;17(41):4614-4618.
doi pubmed - Lee SW, Lien HC, Chang CS, Peng YC, Ko CW, Chou MC. Impact of body mass index and gender on quality of life in patients with gastroesophageal reflux disease. World J Gastroenterol. 2012;18(36):5090-5095.
doi pubmed - Lippmann QK, Crockett SD, Dellon ES, Shaheen NJ. Quality of life in GERD and Barrett's esophagus is related to gender and manifestation of disease. Am J Gastroenterol. 2009;104(11):2695-2703.
doi pubmed - Aro P, Ronkainen J, Storskrubb T, Bolling-Sternevald E, Lind T, Graffner H, Talley NJ, et al. Quality of life in a general adult population with gastroesophageal reflux symptoms and/or esophagitis: A report from the Kalixanda study. Gastroenterology. 2003;124:A168.
doi - Koloski NA, Talley NJ, Boyce PM. The impact of functional gastrointestinal disorders on quality of life. Am J Gastroenterol. 2000;95(1):67-71.
doi pubmed - Wiklund I, Carlsson J, Vakil N. Gastroesophageal reflux symptoms and well-being in a random sample of the general population of a Swedish community. Am J Gastroenterol. 2006;101(1):18-28.
doi pubmed - Ronkainen J, Aro P, Storskrubb T, Lind T, Bolling-Sternevald E, Junghard O, Talley NJ, et al. Gastroesophageal reflux symptoms and health related quality of life in the adult general population - the Kalixandra study. Aliment Pharmacol Ther. 2006;23:1725-1733.
doi pubmed - Jones R, Horbach S, Sander P, Ryden-Bergsten T. Heartburn in patients with gastro-oesophageal reflux disease in Germany and Sweden: a study on patients' burden of disease. Pharmacoeconomics. 2003;21(15):1091-1102.
doi pubmed - Ponce J, Beltran B, Ponce M, Zapardiel J, Ortiz V, Vegazo O, Nuevo J. Impact of gastroesophageal reflux disease on the quality of life of Spanish patients: the relevance of the biometric factors and the severity of symptoms. Eur J Gastroenterol Hepatol. 2009;21(6):620-629.
doi pubmed - Wahlqvist P. Symptoms of gastroesophageal reflux disease, perceived productivity, and health-related quality of life. Am J Gastroenterol. 2001;96(8 Suppl):S57-61.
doi - Kulig M, Leodolter A, Vieth M, Schulte E, Jaspersen D, Labenz J, Lind T, et al. Quality of life in relation to symptoms in patients with gastro-oesophageal reflux disease - an analysis based on the ProGERD initiative. Aliment Pharmacol Ther. 2003;18(8):767-776.
doi pubmed - Yang SY, Lee OY, Bak YT, Jun DW, Lee SP, Lee SH, Park GT, et al. Prevalence of gastroesophageal reflux disease symptoms and uninvestigated dyspepsia in Korea: a population-based study. Dig Dis Sci. 2008;53(1):188-193.
doi pubmed - Tack J, Becher A, Mulligan C, Johnson DA. Systematic review: the burden of disruptive gastro-oesophageal reflux disease on health-related quality of life. Aliment Pharmacol Ther. 2012;35(11):1257-1266.
doi pubmed - Wahlqvist P, Carlsson J, Stalhammar NO, Wiklund I. Validity of a Work Productivity and Activity Impairment questionnaire for patients with symptoms of gastro-esophageal reflux disease (WPAI-GERD) - results from a cross-sectional study. Value Health. 2002;5(2):106-113.
doi pubmed - Dean BB, Crawley JA, Schmitt CM, Wong J, Ofman JJ. The burden of illness of gastro-oesophageal reflux disease: impact on work productivity. Aliment Pharmacol Ther. 2003;17(10):1309-1317.
doi pubmed - Dubois RW, Aguilar D, Fass R, Orr WC, Elfant AB, Dean BB, Harper AS, et al. Consequences of frequent nocturnal gastro-oesophageal reflux disease among employed adults: symptom severity, quality of life and work productivity. Aliment Pharmacol Ther. 2007;25(4):487-500.
doi pubmed - Jones R, Liker HR, Ducrotte P. Relationship between symptoms, subjective well-being and medication use in gastro-oesophageal reflux disease. Int J Clin Pract. 2007;61(8):1301-1307.
doi pubmed - Wahlqvist P, Reilly MC, Barkun A. Systematic review: the impact of gastro-oesophageal reflux disease on work productivity. Aliment Pharmacol Ther. 2006;24(2):259-272.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.